485 - Cytomegalovirus (CMV) Infection in Very-Low-Birth-Weight (VLBW) Infants: Unraveling the Difference Between Congenital and Postnatal Infections
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3467.485
Abigail Parro, Nationwide Children's Hospital, Columbus, OH, United States; Sebastian Martinez, Nationwide Children's Hospital, Columbus, OH, United States; Traci Pifer, Nationwide Children's Hospital, Columbus, OH, United States; Holly T. Gerth, Nationwide Children's Hospital, Columbus, OH, United States; Ursula M.. Findlen, Nationwide Children's Hospital, Columbus, OH, United States; Sara Conroy, Nationwide Children's Hospital, Columbus, OH, United States; Chance Alvarado, Nationwide Children's Hospital, Columbus, OH, United States; Masako Shimamura, Nationwide Children's Hospital, Columbus, OH, United States; Oliver F. Adunka, The Ohio State University, Columbus, OH, United States; Prashant Malhotra, Nationwide Children's Hospital, Columbus, OH, United States; Zachery S. Lewald, Nationwide Children's Hospital, Columbus, OH, United States; Pablo J. Sanchez, Nationwide Children's Hospital -OSU, Columbus, OH, United States
Resident Nationwide Children's Hospital Columbus, Ohio, United States
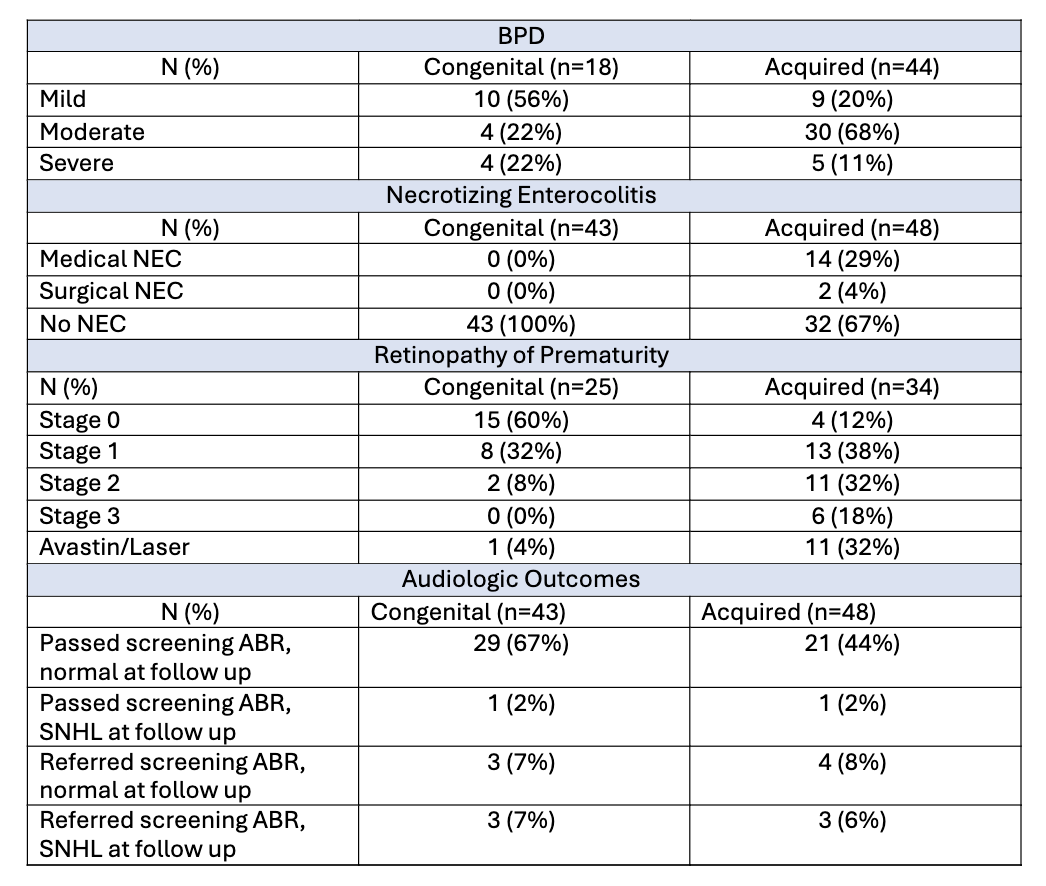
Background: Postnatally-acquired CMV infection contributes substantially to morbidity and mortality in preterm VLBW infants in the NICU. Distinguishing postnatal from congenital CMV infection is challenging due to lack of universal CMV birth screening in most NICUs. In addition, the clinical management of each type of CMV infection varies, and the outcomes of VLBW infants with acquired CMV, especially sensorineural hearing loss (SNHL), are uncertain. In the 9 Columbus, OH NICUs, all admissions are tested for CMV to inform practice and ascertain postnatally-acquired disease. Objective: To compare demographic, clinical, laboratory, and NICU outcomes of VLBW infants with congenital vs. postnatally-acquired CMV infection. Design/Methods: This retrospective analysis included VLBW infants admitted to 9 NICUs in Columbus, OH, who were diagnosed with congenital or acquired CMV from 2010-2025. Congenital infection was defined as a positive urine or newborn dried blood spot CMV PCR at < 21 days of age. Acquired CMV was defined as a negative saliva/urine CMV PCR at < 21 days but subsequent positive urine/blood CMV PCR. Demographic, clinical, laboratory, audiologic, and outcome data of infants with congenital vs. postnatal CMV infection were compared. Results: During the 16 year study, 91 VLBW infants had CMV infection with 43 (47%) having congenital and 48 (53%) postnatal infection (Table 1). Most infants with congenital and acquired CMV infection were female (51% vs. 56%, respectively). Most infants with congenital infection were Black (47%) while most of the acquired cases were White (44%). CMV viral load was higher among infants with postnatal CMV infection (Table 1). Maternal breast milk was received by 90% (n=43) of postnatally CMV-infected infants. Antivirals were provided to 27 (63%) congenital and 11 (23%) postnatal cases. In the congenital CMV cohort, 6 (14%) infants referred on the newborn hearing screen; 3 (7%) had SNHL requiring cochlear implants, and 1 (2%) developed late-onset SNHL (Table 2). Among postnatally-acquired cases, 11 (23%) infants referred on the newborn hearing screen; 3 (6%) had SNHL and 1 (2%) had late-onset SNHL. Infants with postnatal CMV infection had more BPD, NEC, and ROP (Table 2; P< 0.05). Two (4%) infants with acquired CMV and 4 (9%) patients with congenital CMV infection died.
Conclusion(s): Postnatally-acquired CMV infection was associated with more neonatal adverse outcomes than congenital infection. SNHL did not differ among infants with congenital vs. postnatal infection. Universal CMV screening of NICU admissions may aid in understanding the contribution of acquired CMV infection to SNHL.
Table 1. Clinical Characteristics and CMV Testing of Study Population
Table 2. Neonatal Outcomes and Sensorineural Hearing Loss Among VLBW Infants with Congenital vs. Postnatally Acquired CMV Infection

 photo")
.png)