487 - Congenital Cytomegalovirus Screening: Targeted vs. Expanded
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3469.487
Mia Bersalona, Rutgers New Jersey Medical School, Manasquan, NJ, United States; Onajovwe O. Fofah, Rutgers New Jersey Medical School, Newark, NJ, United States; Salma Ali, NJMSD/Rutgers, Saddle River, NJ, United States; Adaora G. Madubuko, Rutgers New Jersey Medical School, Livingston, NJ, United States; Areej Qadri, Rutgers New Jersey Medical School, West Orange, NJ, United States; Nicole M. Raia, Rutgers University, Newark, NJ, United States; Rani Thomas, University hospital Newark , NJ, Newark, NJ, United States; Harpreet Kaur, Rutgers New Jersey Medical School, North Brunswick, NJ, United States
Medical Student Rutgers New Jersey Medical School Manasquan, New Jersey, United States
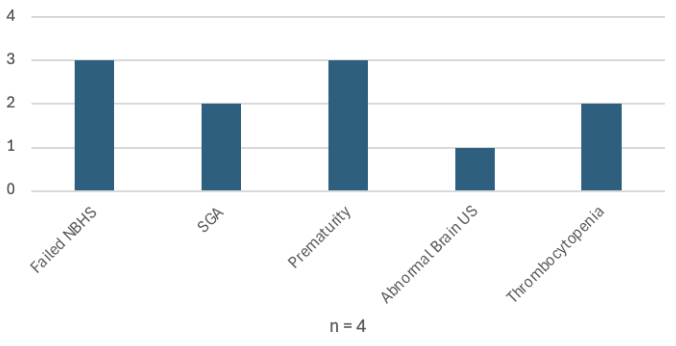
Background: Cytomegalovirus is a double-stranded herpesvirus that can be transmitted to newborns transplacentally, during birth, and through breastfeeding. According to the CDC, congenital cytomegalovirus (cCMV) occurs in approximately 1 in 200 livebirths and is the most common non-genetic cause of congenital hearing loss. Since this is a progressive sensorineural hearing loss (SNHL), early detection and intervention are critical for improved outcomes. Targeted screening, in which testing is reserved for those who fail newborn hearing screening (NBHS), provides a cost-effective method by which to screen at-risk infants. Expanded-targeted screening aims to capture a wider range of affected newborns - common criteria include small for gestational age (SGA), microcephaly, thrombocytopenia, and growth impairment. The gold standard for diagnosis is urine culture or PCR within the first 21 days of life. Objective: Improve outcomes of newborns with cCMV by early detection and treatment in an academic tertiary medical center in Newark, New Jersey. Design/Methods: Beginning October 2022, urine CMV culture testing was implemented as standard of care for all newborns who failed Newborn Hearing screen (NBHS) at University Hospital in Newark, New Jersey. Additionally, some infants who were identified as small for gestational age (SGA) underwent urine CMV testing as part of their evaluation. Newborns that failed NBHS were referred for repeat audiology assessment with Auditory Brainstem Response in two weeks. Results: We had 4 positive cases with a total N=222 newborns that were tested for cCMV. Cases #1 and 2 failed NBHS. Case #3 was SGA with abnormal prenatal neurological abnormalities and failed NBHS. Case #4 was SGA and passed NBHS (Table 1 and Graph 1).
Conclusion(s): The results support use of expanded-targeted screening to capture affected newborns that may be otherwise missed by hearing-targeted screening alone. Criteria may be expanded to include premature infants and those small for gestational age. Broader screening criteria may facilitate early detection and treatment to slow or prevent progressive SNHL.


.png)