109 - Ready, Set, Discharge: Improving NICU Discharge Efficiency and Reducing Parental Burden
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3104.109
Nicole T. Spillane, Hackensack University Medical, Bronxville, NY, United States; joanne Pasinski, Joseph M. Sanzari Children's Hospital Hackensack University Medical Center, Hackensack, NJ, United States; Anamika Desai, Hackensack Meridian Health, Old Bridge, NJ, United States; Maureen Kim, Joseph M. Sanzari Children's Hospital Hackensack University Medical Center, Hackensack, NJ, United States
Associate Professor Hackensack University Medical Bronxville, New York, United States
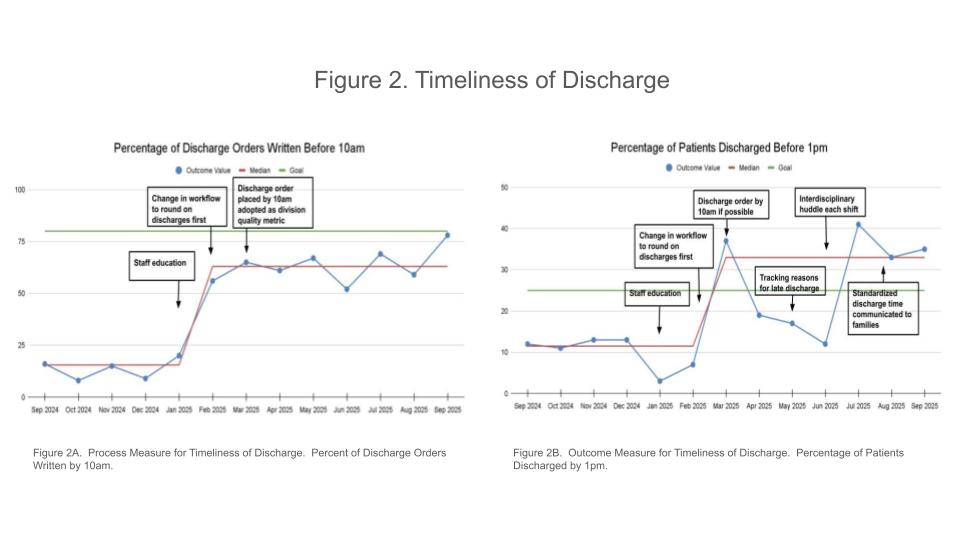
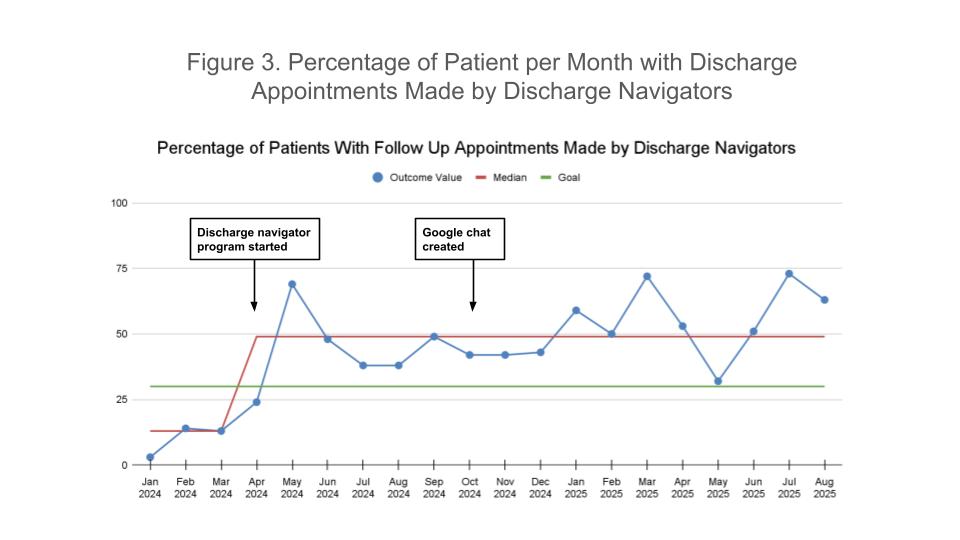
Background: Optimizing NICU discharge improves parental satisfaction, reduces overcrowding, and improves hospital costs. Despite these benefits, multiple barriers in the discharge process exist. Objective: Improve the discharge process by improving discharge timeliness and by reducing the family burden of scheduling discharge appointments. Aim 1: Improve discharge time before 1pm from a baseline of 11.5% to 25% by December 2025. Aim 2: Increase the percentage of patients with outpatient specialty appointments scheduled by discharge coordinators from a baseline of 13% to 30% by December 2025. Design/Methods: A multidisciplinary QI team was formed in 2023. PDSA cycles starting in Jan 2025 to improve timeliness of discharge included: (1) staff education, (2) expectation for discharge orders by 10am, (3) tracking reasons for late discharge (Figure 1), (4) shift huddles to address barriers to early discharge, and (5) communication to families about discharge time. PDSA cycles starting in Jan 2024 to improve scheduling of outpatient appointments included: (1) establishing a program with discharge navigators coordinating with parents and scheduling discharge appointments and (2) creating a google chat to facilitate communication with discharge navigators. Our outcome measures included percentage of discharges before 1pm and percentage of patients with appointments made by discharge navigators. Our process measure was the percentage of discharge orders placed by 10am. Results: The percentage of patients discharged before 1pm increased from 11.5% during our baseline period to 33% during our intervention period, with a sustained increase to ≥33% for the last 3 months (Figure 2). The percentage of discharge orders placed by 10am improved significantly from 15.5% to 63% (Figure 2), with an improvement in the median time of discharge order from 12:11pm to 9:45am. The percentage of patients who had outpatient appointments scheduled by discharge navigators increased from 13% to 49% (Figure 3).
Conclusion(s): Our QI project was able to improve the timeliness of our NICU discharges and reduce parental burden by providing assistance with scheduling outpatient appointments. This initiative is ongoing, and future plans include posting signage to indicate discharge time for the parents, streamlining the circumcision process, and surveying parents about their satisfaction with the discharge process and their sense of preparedness for discharge. We also plan to evaluate the effects of our early discharge initiative on NICU length of stay and readmission rates and the effects of appointment scheduling on outpatient follow up rates.
Pareto Chart for Discharge Delays
Timeliness of Discharge
Percentage of Patients Per Month with Discharge Appointments Made by Discharge Navigators

 Credit")
 photo")
.jpg)