139 - Implementing Minimally Invasive Surfactant Therapy at McMaster Children’s Hospital’s NICU: A pre- and post-implementation cohort study
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3133.139
Amit Mukerji, McMaster University, Hamilton, ON, Canada; Sayem Borhan, McMaster University, Hamilton, ON, Canada; Rana Sutton, McMaster University Michael G. DeGroote School of Medicine, Ancaster, ON, Canada; Laura Armstrong, Hamilton Health Sciences, Cambridge, ON, Canada; Melanie Amyotte, Hamilton Health Science, Hamilton, ON, Canada; Jennifer Twiss, McMaster University Michael G. DeGroote School of Medicine, Ancaster, ON, Canada; Kristian Ashali, McMaster University Michael G. DeGroote School of Medicine, Hamilton, ON, Canada
Associate Professor McMaster University Hamilton, Ontario, Canada
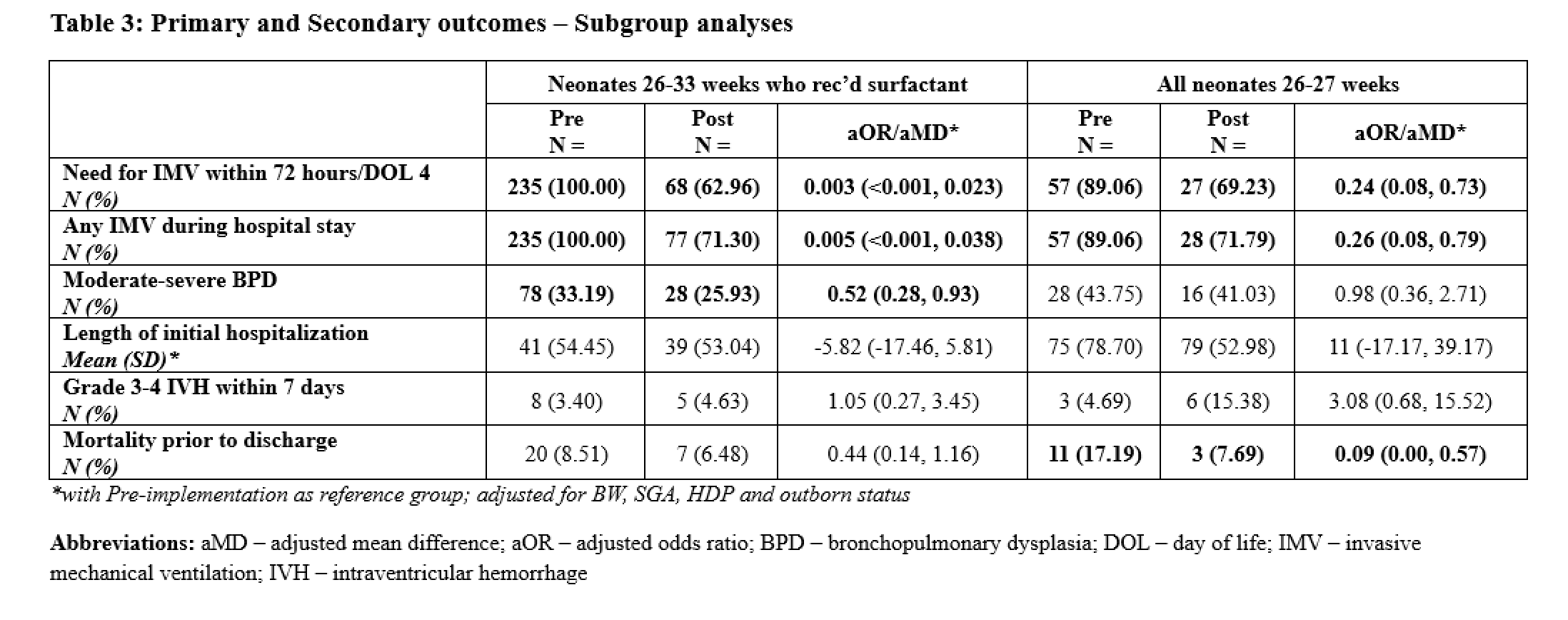
Background: Minimally invasive surfactant therapy (MIST) is an alternate method of surfactant administration for preterm infants. Evidence suggests that MIST may reduce the need for invasive mechanical ventilation (IMV), decrease bronchopulmonary dysplasia (BPD), and lower the rate/severity of intraventricular hemorrhage (IVH) compared to traditional methods. Objective: To evaluate the real-world impact of MIST implementation in the NICU at McMaster Children's Hospital. Design/Methods: A MIST guideline was adopted for infants 26-33 weeks' gestational age (GA) and implemented in 2 phases (28-33 weeks GA and 26-27 weeks GA in April 2023 and March 2024, respectively). The primary (IMV within 72 hours) and secondary outcomes (moderate-severe BPD and adverse events such as mortality and IVH) were compared between the pre- (2 years) and post- (1 year) implementation periods for all admitted neonates 26-33 weeks' GA. Subgroup analyses were done for: 1) infants 26-33 weeks' GA who received surfactant; and 2) neonates 26-27 weeks' GA (regardless of surfactant administration). Regression models adjusted for potential confounders; P value < 0.05 was considered significant. Results: 819 infants were included in the study - 591 (235 received surfactant) and 228 (108 received surfactant, of whom 54 received MIST based on eligibility criteria) were in the pre- and post-implementation periods, respectively. Baseline and demographic characteristics were comparable (Table 1). When comparing all infants, IMV within 72 hours was needed in 35% vs 47% (aOR 0.51 [0.36, 0.72] P< 0.001) in the post- vs pre-implementation periods. Moderate-severe BPD was lower post-implementation (22% vs 26% aOR 0.60 [0.38, 0.92] P=0.021). When restricted to infants who had received surfactant, IMV within 72 hours was needed in 63% vs 100% (aOR 0.003 [ < 0.001, 0.023] P< 0.001) in the post- vs pre-implementation periods. Moderate-severe BPD was lower post-implementation: 26% vs 33% (aOR 0.52 [0.28, 0.93] P=0.032). In neonates 26-27 weeks' GA (regardless of surfactant, N=39 post and N=64 pre-implementation) IMV within 72 hours was needed in 69% vs 89% (aOR 0.24 [0.08, 0.073] P=0.013). However, no difference in moderate-severe BPD was seen: 41% vs 44%, aOR 0.98 (0.36, 0.79) P=0.97). Detailed results shown in Tables 2&3. No differences in adverse effects were noted across any of the cohorts.
Conclusion(s): MIST significantly reduced the need for IMV within 72 hours of life without increased adverse effects, supporting its broader adoption as a standard of care in the NICU. Further data on short- and long-term outcomes in extremely preterm neonates is required.
Table 1: Baseline and demographic characteristics
Table 2: Primary and Secondary outcomes - Main cohort (All neonates 26-33 weeks' GA)
Table 3: Primary and Secondary outcomes - Subgroup analyses

.png)
.png)