573 - Post-cardiac arrest management and physiology in a Level IV NICU after implementation of a clinical guideline
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3554.573
Mary Haggerty, Children's Hospital of Philadelphia, haddonfield, NJ, United States; Kristen Coletti, Children's Hospital of Philadelphia, Wynnewood, PA, United States; Heidi M. Herrick, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Anne Ades, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Laura Sillers, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Lauren Heimall, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Sarah A. Coggins, Children's Hospital of Philadelphia, Philadelphia, PA, United States
Attending Neonatologist Children's Hospital of Philadelphia haddonfield, New Jersey, United States
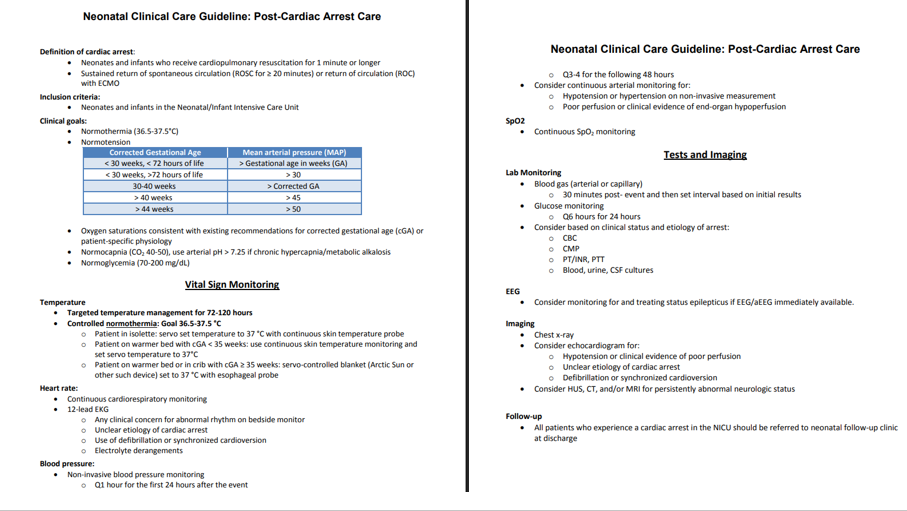
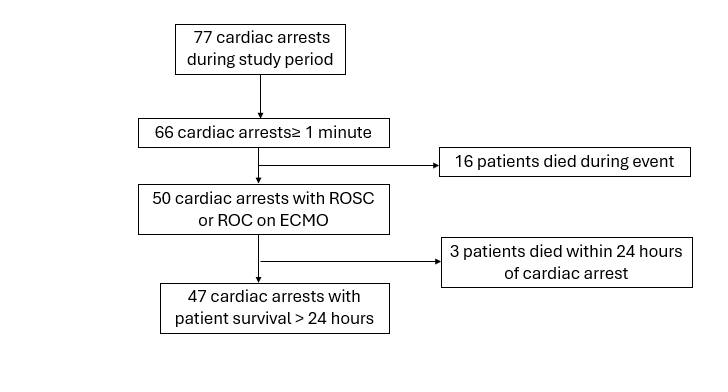
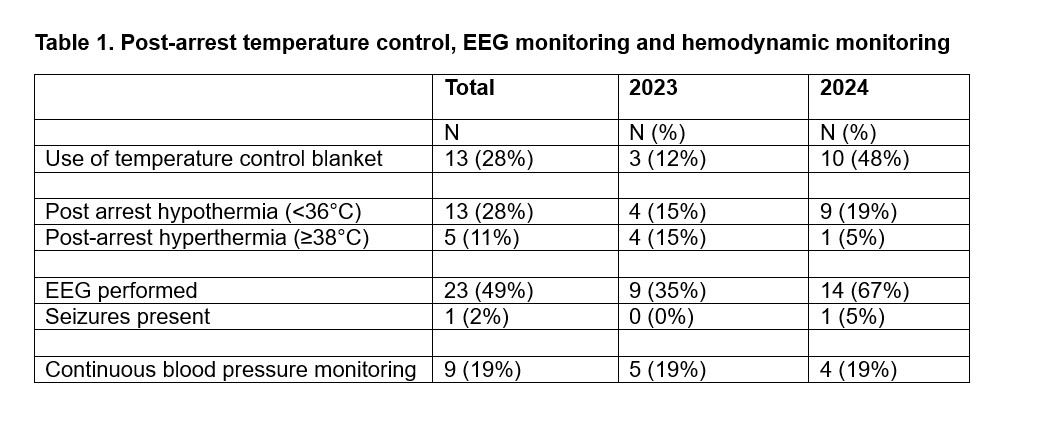
Background: High-quality post-cardiac arrest care is critical to optimize outcomes. The American Heart Association (AHA) Pediatric Advanced Life Support (PALS) guidelines provide specific recommendations for post-cardiac arrest care in the pediatric population. Our previous study in a single academic Level IV NICU showed substantial variability in post-cardiac arrest practices and a high rate of hypothermia. In April 2022, we developed consensus guidelines for the NICU based on AHA recommendations (Figure 1). Objective: To describe post-cardiac arrest care practices and clinical outcomes after clinical guideline development from April 2022 to December 2024. We excluded the first 8 months as an implementation period. Design/Methods: Single center retrospective observational study of patients who received 1 minute of chest compressions in the CHOP NICU with ROSC or ROC on ECMO and survived for at least 24 hours after cardiac arrest from 1/1/2023 to 12/31/2024. Patients and resuscitation characteristics were identified in a hospital QI resuscitation database. Additional post-arrest data was obtained from the electronic health record. Descriptive statistics were used to summarize post-arrest practices. The primary outcome is adherence to clinical guidelines (temperature control with normothermia using temperature control blanket, EEG, and continuous blood pressure monitoring). Secondary outcomes are hypo- or hyperthermia within 24 hours after arrest and the presence of seizures. Results: There were 66 cardiac arrests ≥ 1 minute during the study period. There were 47 events with patient survival >24 hours (Figure 2). There were 7 patients with >1 cardiac arrest, all of which occurred >24 hours apart. Overall guideline compliance for use of continuous core temperature monitoring and temperature control blanket (28%), EEG (49%) and continuous blood pressure monitoring (19%) was low but improved over time (Table 1). 28% of patients had at least one episode of hypothermia ( < 36°C), 11% had at least one episode of hyperthermia (≥38°C) and 1 patient (2%) experienced seizures in the first 24 hours after cardiac arrest.
Conclusion(s): In the first 32 months after post-cardiac arrest care guideline development, overall guideline compliance was low but improved over the study period. Despite clinical guideline development, 28% of cardiac arrest survivors experienced post-arrest hypothermia. There is opportunity for more robust implementation methodology to improve guideline compliance and hypothermia rates.
Figure 1. NICU post-cardiac arrest care guidelines
Figure 2. Diagram of outcomes of cardiac arrest events
Table 1. Post-arrest temperature control, EEG monitoring and hemodynamic monitoring