111 - Virtual Human Factors Table-top Evaluations to Improve Neonatal Resuscitation in Rural Hospitals
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3106.111
Brenda H. Law, University of Alberta, Edmonton, AB, Canada; Jared Dembicki, Alberta Health Services, Edmonton, AB, Canada; Shaunna Milloy, Alberta health services, Calgary, AB, Canada; Megan E. Rolleman, Alberta Health Services, Edmonton, AB, Canada; Krystyna Ediger, University of Alberta Faculty of Medicine and Dentistry, Edmonton, AB, Canada
Assistant Professor University of Alberta Edmonton, Alberta, Canada
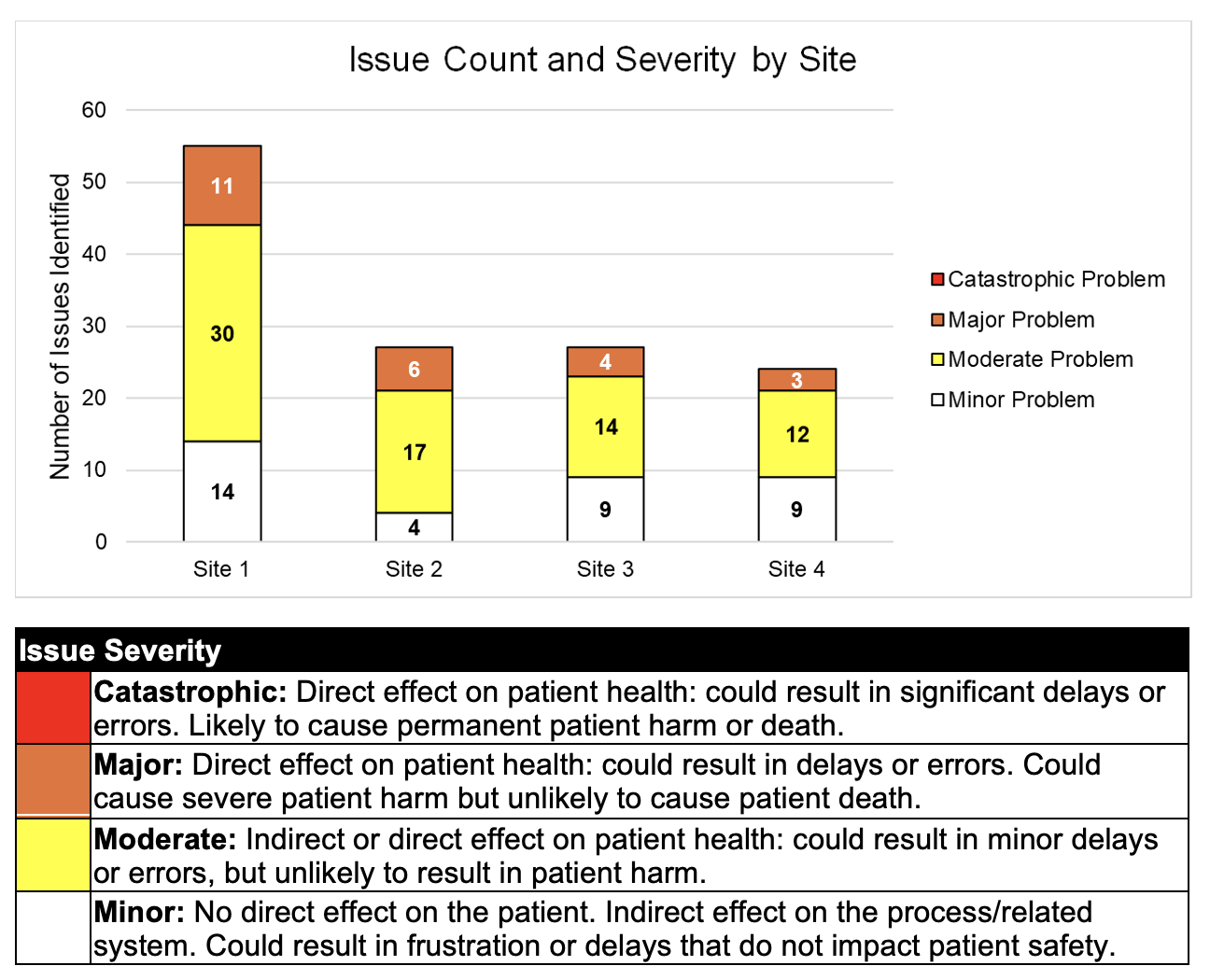
Background: Tertiary centers can support neonatal resuscitation and stabilization (NRS) in rural locations via telehealth. Telehealth can also connect academic experts with community hospitals for quality improvement, allowing outreach programs to assist with improving health systems factors such as equipment, physical spaces, and processes -elements related to human factors (HF). The Systems Engineering Initiative for Patient Safety (SEIPS) model provides a HF framework for examining interactions between system elements (i.e. person, tasks, tools and technologies, physical environment, and organization), processes, and outcomes. Virtual tabletop simulations conducted via teleconference, informed by SEIPS, may be helpful for neonatology and rural healthcare teams to identify NRS quality improvement targets. Objective: To use virtual tabletop simulations to evaluate human factors issues related to neonatal resuscitation and stabilization in rural hospitals. Design/Methods: Hospitals participated as a part of a needs assessment for a tele-outreach program led by their perinatal referral center. First, neonatologists, HF and simulation experts met with site stakeholders to discuss goals, current capabilities and challenges. Then, scenarios were developed for each site, related to one of: hypoxic ischemic encephalopathy, respiratory distress, or preterm birth. Tabletop simulations were conducted virtually using Zoom or Microsoft Teams videoconferencing, with Microsoft Whiteboard as an interactive platform showing scenario information, hospital floor plans, and images of physical spaces.(Figure 1) After pre-brief, participants talked through scenario steps, explaining clinical tasks, key decisions, communication pathways, tools, and hazards. A debrief using semi-structured questions mapped to SEIPS categories elicited further information on successes and challenges. Notes and video recordings were analyzed to generate lists of system issues which could impact NRS. Issues were rated by severity and categorized by SEIPS work system components. Results: 21 clinicians from 4 sites participated. No catastrophic issues were identified.(Figure 2) Issues were mapped to SEIPS categories.(Table 1) Recurrent themes pertain to: difficulties with neonatal intubation, laryngeal mask airways, and umbilical venous catheters; need for triggers for telehealth and transport activation; telehealth equipment limitations; limitations in staffing in rural sites; and need for cognitive aids.
Conclusion(s): Virtual table-top simulations underpinned by SEIPS is a powerful tool to identify quality improvement targets for NRS in rural settings.
Figure 1. Screen shot of Virtual Table-top Environment
Figure 2. Issues by Severity Rating
Table 1. Key challenges and examples for each SEIPS work system category.

 photo")
.png)
.png)
