Alicia M. Lim, KK Women's and Children's Hospital, Singapore, N/A, Singapore; Juin Yee Kong, KK Women's and Children's Hospital, Singapore, N/A, Singapore; Kee Thai Yeo, KK Women's & Children's Hospital, Singapore, N/A, Singapore; Georg Schmolzer, University of Alberta Faculty of Medicine and Dentistry, Edmonton, AB, Canada; Siyuan Jiang, Children's Hospital of Fudan University, Shanghai, Shanghai, China (People's Republic); Han-Suk Kim, Seoul National University Children's Hospital, Jongno-Gu, Seoul-t'ukpyolsi, Republic of Korea; Lloyd J. Tooke, University of Cape Town, Cape Town, Western Cape, South Africa; Janneke Dekker, Leiden University Medical Center, Leiden, Zuid-Holland, Netherlands; Victor Javier Lara-Diaz, UNSW, Monterrey, Nuevo Leon, Mexico; Danielle Trevisanuto, University of Padova, Padova, Veneto, Italy; Elizabeth SF. Chong, RIPAS Hospital Brunei, Bandar Seri Begawan, Brunei and Muara, Brunei; Maria Lourdes S. Imperial, Dr. Jose Fabella Memorial Hospital, Pasig City, National Capital Region, Philippines; Henry Lee, University of California San Diego, La Jolla, CA, United States; Srabani Samanta, Manchester University NHS Foundation Trust, Manchester, England, United Kingdom; Reza Syahputra, Dr. Sardjito Hospital, Yogyakarta, Yogyakarta, Indonesia; Ju Lee Oei, Mater Research, South Brisbane, Queensland, Australia
Senior Consultant KK Women's & Children's Hospital Singapore, Singapore
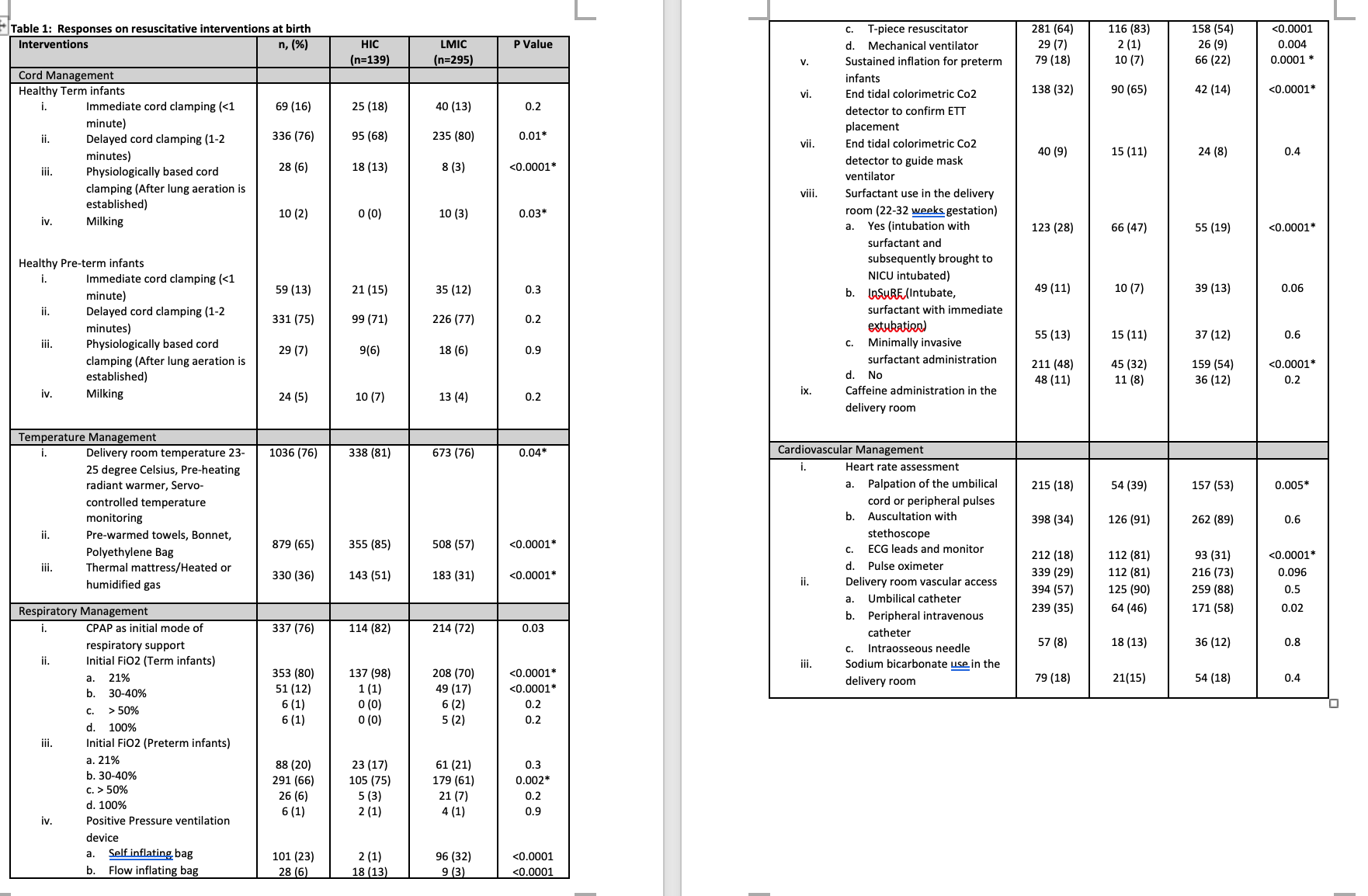
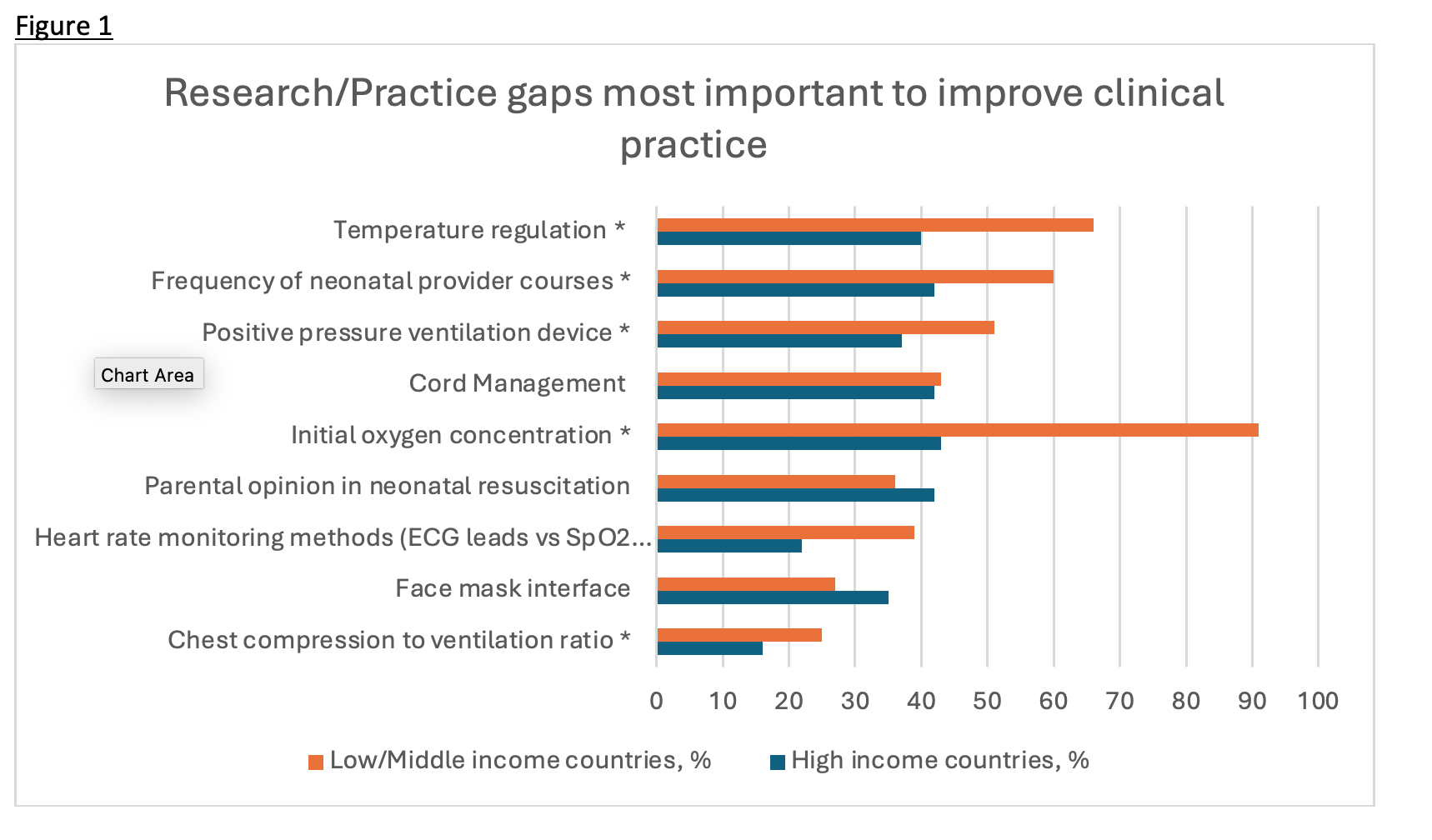
Background: As many as 16% of infants need some form of assistance immediately after birth. Although neonatal resuscitation is a common occurrence, the extent and variations in clinical practice across regions are not well characterised. Objective: To assess the global usage patterns of various neonatal resuscitation interventions and to explore healthcare professionals' perspectives on the key life-saving interventions. We hypothesize that practices and priorities differ significantly according to individual resource context and regional practice environments. Design/Methods: An anonymous, IRB-approved, web-based survey via Microsoft Forms was administered to healthcare practitioners engaged in neonatal resuscitation from 37 countries, between April to October 2025. Statistical analyses were stratified by country-specific income levels using the World Bank classifications. Results: We received 436 responses - 142 (31%) from high-income countries (HIC) and 295 (65%) from low- and middle-income countries (LMIC). Most respondents (48%) worked in Level III neonatal intensive care units with annual delivery rates of < 2000 births. The lowest reported median gestational age for commencing resuscitation was 22 weeks for HIC compared to 24 weeks for LMIC. HIC respondents were more inclined to perform physiologically based cord management for term infants compared to LMIC (13% versus 3%, p< 0.001) (Table 1). Initial respiratory support using continuous positive airway pressure (CPAP) was more prevalent in HIC compared to LMICs (82% vs 72%, p=0.03). For term infants, almost all HIC respondents were more likely to start resuscitation at 21% FiO2. Of note, sustained inflation techniques was more commonly employed in LMICs (22% versus 7%, p=0.0001). End-tidal CO2 colorimetric detection was predominantly used in HICs (65% versus 14%, p< 0.0001). The three highest-ranked interventions for preventing mortality were positive pressure ventilation devices, temperature regulation, and face mask interfaces. Research practice gaps that practitioners considered most critical for enhancing clinical practice were initial oxygen concentration, temperature regulation, and neonatal provider training frequency (Figure 1).
Conclusion(s): Variation in resuscitative practices exist worldwide. HIC were more likely to do physiologically based cord clamping, use T piece to administer CPAP in the delivery room, use end-tidal colorimetric monitoring and start resuscitation with room air in term infants. These variations may be due resource disparities among the different settings.
Table 1: Summary of resuscitative measures at birth
Figure 1: Research/Practice Gaps Most important to improve clinical practice