36 - How We Give a “High Five for P-5" and Build Sustainable Early Childhood Developmental and Behavioral Health Services in Primary Care: Insights from a Landscape Analysis
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3033.36
Claire E.. Kingsbury, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Amie Bettencourt, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Mackenzie J. Simon-Collins, Drexel University College of Medicine, Jacksonville, FL, United States; Angela Suarez, Johns Hopkins University School of Medicine, Washington DC, DC, United States; Eliana M.. Perrin, Johns Hopkins University School of Medicine, Baltimore, MD, United States
Senior Research Coordinator Johns Hopkins University School of Medicine Baltimore, Maryland, United States
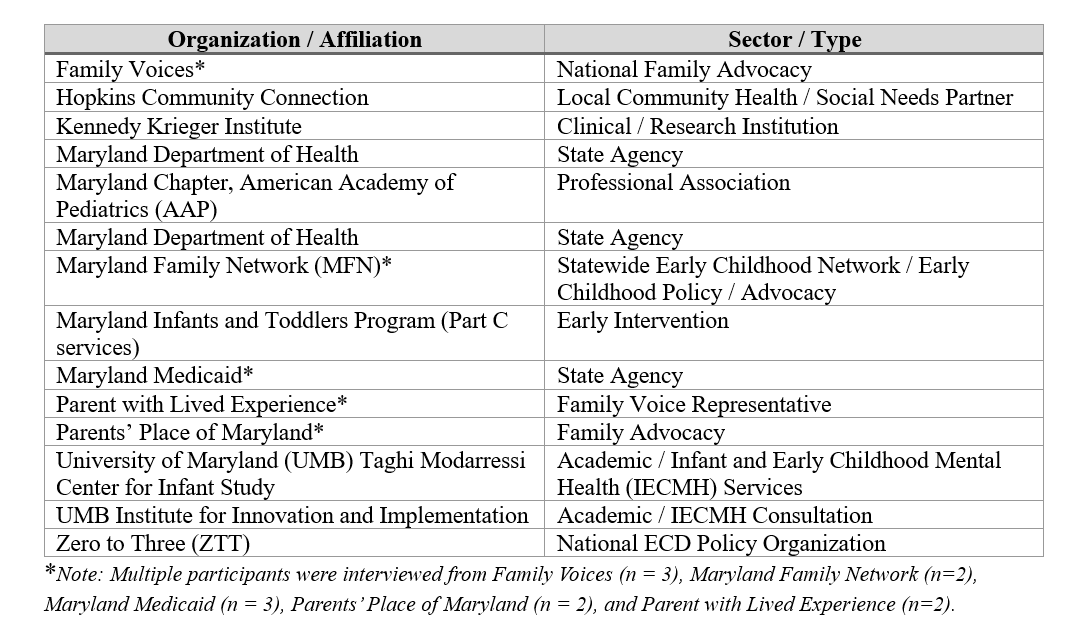
Background: Integrating early childhood developmental and behavioral health (ECDBH) services into primary care is essential for improving young children's developmental, behavioral, and emotional outcomes. Yet, fragmented systems, limited reimbursement, and workforce constraints challenge sustainability. The "High Five for P-5" (Prenatal to Five) project conducted a statewide landscape analysis to identify financing and policy levers to sustain equitable ECDBH services across Maryland. Objective: To examine barriers, opportunities, and policy strategies for sustainable ECDBH integration in primary care. Design/Methods: We conducted 17 semi-structured interviews with 21 stakeholders (see Table 1) from local, state, and national organizations focused on children's health and well-being, including parents with lived experience. Interviews explored barriers and opportunities to ECDBH services and visions for an ideal system. Sessions were held via Zoom, recorded, and transcribed verbatim. Our team used inductive, consensus-based content analysis in Dedoose to identify recurrent themes in service delivery, financing, and sustainability. Results: Six themes emerged: 1) Geographic disparities in access and service quality, notably for rural families; 2) Fragmented coordination among health, education, and social systems causing duplicative efforts; 3) Limited awareness of available services among families and providers; 4) Referral challenges, including inconsistent referral processes and lack of reimbursement for navigation; 5) Funding and billing barriers, such as diagnosis-dependent reimbursement, inability to bill Z-codes, and exclusions of enhanced payment for Federally Qualified Health Centers; and, 6) A shared vision for a sustainable ECDBH system, coordinated, family-centered services where primary care centrally connects across sectors. One participant explained the current landscape, "You're not going to just make one call that will connect you to everything, you're going to have to make a thousand calls." See Table 2 for thematic quotes.
Conclusion(s): Findings highlight systemic barriers and financing gaps impeding sustainable ECDBH integration in primary care. Policy opportunities include expanding Medicaid enhanced payments, authorizing preventive Z-code billing, and adopting developmentally appropriate diagnostic frameworks (e.g., DC:0-5 Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood). Strengthening cross-sector coordination and equitable funding mechanisms are critical to sustaining comprehensive ECDBH systems statewide with broader national implications.
Table 1. Participating Organizations Represented in the Landscape Analysis

 photo")
.png)
