558 - Advanced resuscitation at birth and critical hospital outcomes in very preterm infants: are there differences among national networks?
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3539.558
Ruth Guinsburg, Universidade Federal de São Paulo, São Paulo, Sao Paulo, Brazil; Maria Fernanda de Almeida, Universidade Federal de Sao Paulo - Brazil, São Paulo, Sao Paulo, Brazil; Yi-Chen Su, mount sinai hospital, Toronto, ON, Canada; Marc Beltempo, McGill University, Montreal, PQ, Canada; Liisa Lehtonen, Turku University Hospital, Turku, Varsinais-Suomi, Finland; Kjell Helenius, University of Turku and Turku University Hospital, Turku, Varsinais-Suomi, Finland; Gil Klinger, Schneider Children's Medical Center of Israel and Tel Aviv University, Ramat Hasharon, Tel Aviv, Israel; Maximo Vento, Instituto de Investigación Sanitaria La Fe (IISLAFE), Valencia, Comunidad Valenciana, Spain; Mikael Norman, Karolinska Institutet, Stockholm, Stockholms Lan, Sweden; Lars Naver, Karolinska universitetssjukhuset, Stockholm, Stockholms Lan, Sweden; Mark Adams, University Hospital Zurich, Zurich, Zurich, Switzerland; Dirk Bassler, University of Zurich, Zurich, Zurich, Switzerland; Vieri Lastrucci, Meyer Children's hospital irccs, Firenze, Toscana, Italy; Neena Modi, Imperial College London, London, England, United Kingdom; Prakesh S Shah, Mount Sinai Hospital, Toronto, ON, Canada
Professor of Pediatrics Universidade Federal de São Paulo Universidade Federal de São Paulo São Paulo, Sao Paulo, Brazil
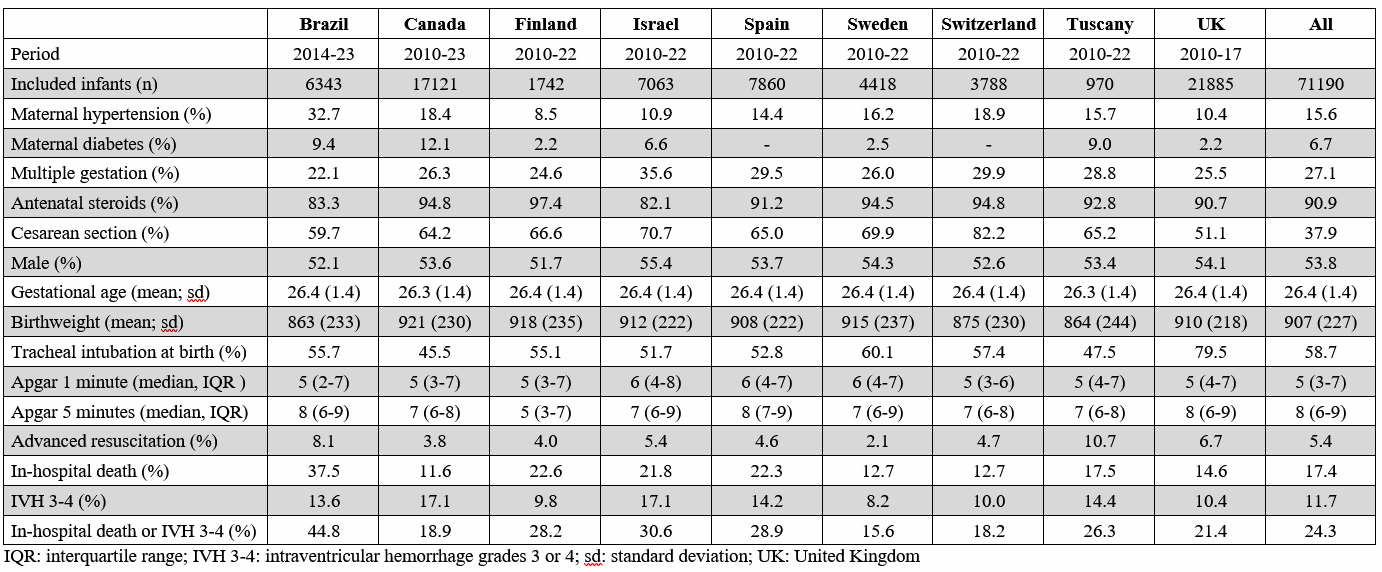
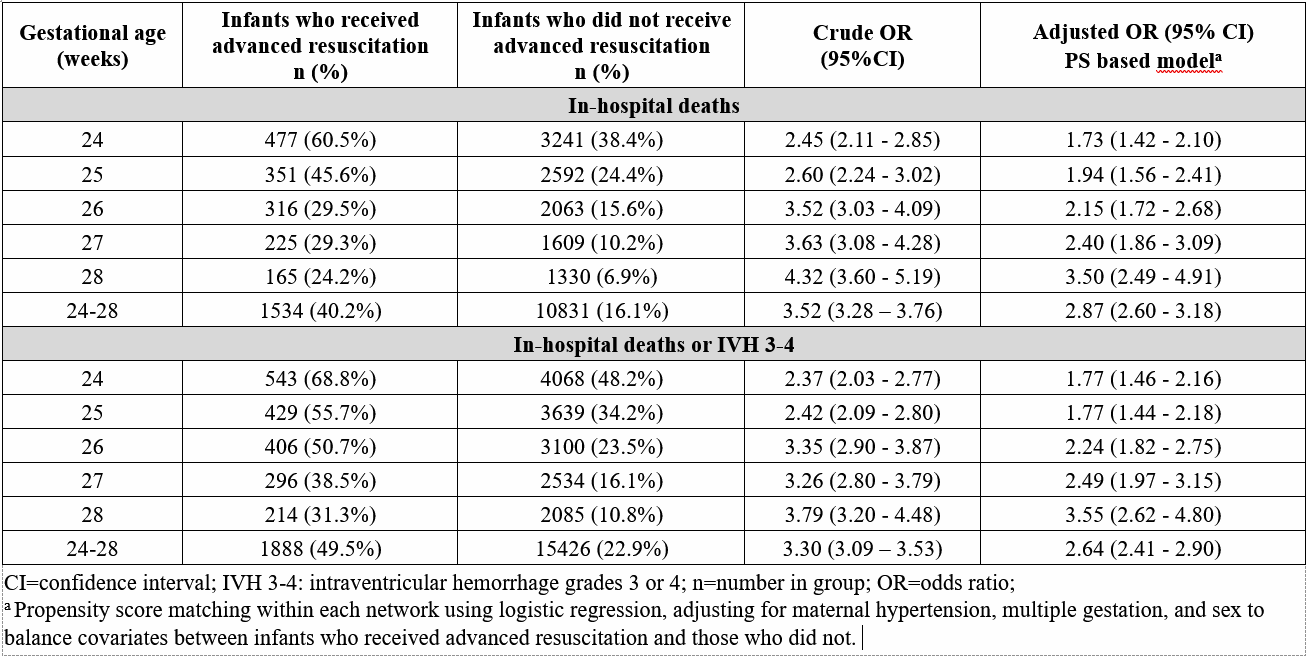
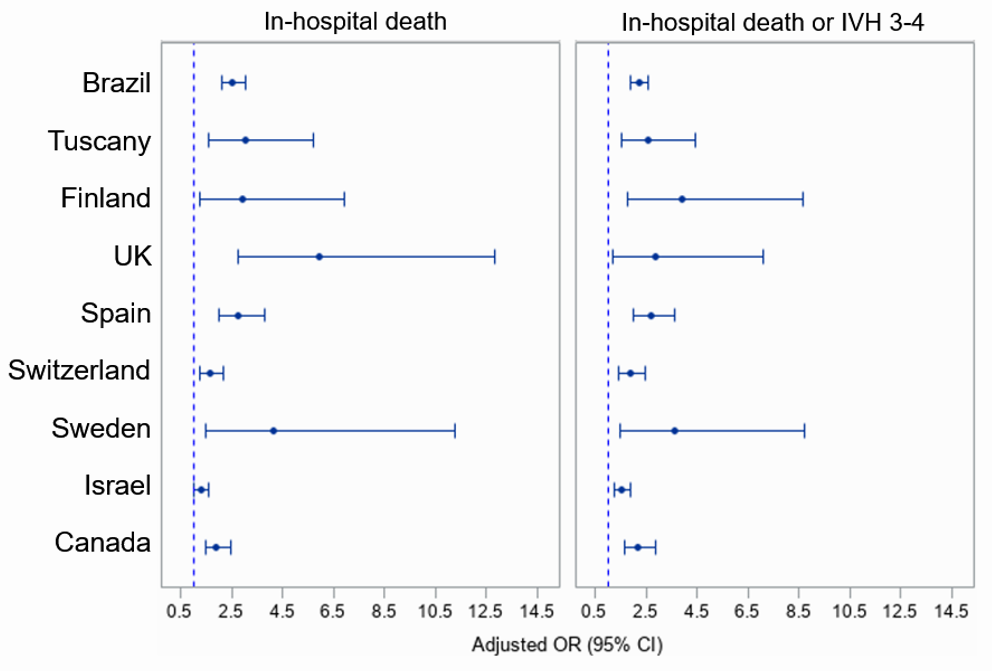
Background: Multicenter studies in very low birth weight preterm infants receiving chest compressions and/or medications at birth show worse outcomes related to morbidity and mortality. It is not known whether the strength of these associations is consistent across different gestational ages and national/regional networks. Objective: To compare, in inborn very preterm neonates who did vs. did not receive advanced resuscitation, the outcomes of in-hospital deaths and the composite of in-hospital death or intraventricular hemorrhage grades 3 or 4 (IVH 3-4) across the International Network for Evaluating Outcomes in Neonates (iNeo) database. Design/Methods: Individual-level data from 9 neonatal iNeo networks were retrieved: Brazil, Canada, Finland, Israel, Spain, Sweden, Switzerland, Tuscany-Italy, and United Kingdom. All infants born alive between 24-28 weeks' gestation, with birth weight < 1500g without major congenital malformations, from 2010-2023, were included. Advanced resuscitation was defined as positive pressure ventilation and chest compression with/without epinephrine administration. Propensity score (PS) matching was stratified by networks. Matching the PS among infants with and without advanced resuscitation (1:1) was based on a caliper width of 0.2 times the standard deviation of the logit-transformed PS. Association between advanced resuscitation and outcomes in each matched sample was analyzed by logistic regression, with generalized estimating equations with an unstructured correlation. Results: Among 84,392 infants with 24-28 weeks gestation and birthweight < 1500g, 71,190 met inclusion criteria and 3812 received advanced resuscitation (5.4%). Characteristics of included infants are shown in Table 1. Infants that received advanced resuscitation had 2.87 and 2.64 higher adjusted odds respectively of in-hospital death and of the composite outcome. For both outcomes, the odds ratio increased with each additional week of gestational age (Table 2). Although the odds of in-hospital death or the composite outcome were higher in each network for infants receiving advanced resuscitation, some variation of adjusted odds ratio was noted among networks (Figure).
Conclusion(s): This study, with a large number of very preterm infants, shows that the strength of the association between receiving advanced resuscitation and critical outcomes varies among different networks and that the strength of this association is higher as gestational age increases. Looking for explanatory factors for these phenomena may help to improve outcomes of this population.
Table 1. Baseline characteristics of included newborn infants
Table 2. Main outcomes in infants who received advanced resuscitation or not by gestational age
Figure. Outcomes for each network from propensity score matching and logistic with generalized estimating equations for network

 photo")