Pediatric Resident Nemours Children's Hospital Orlando, Florida, United States
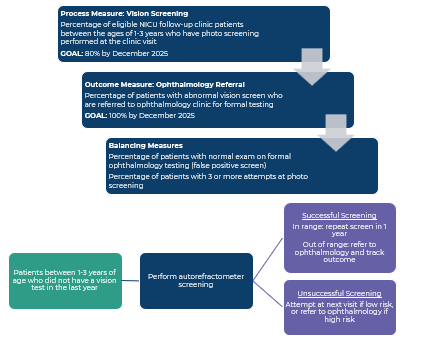
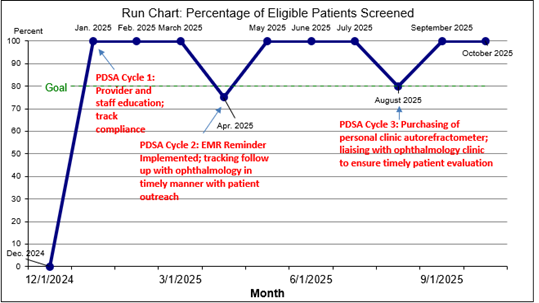
Background: Children requiring neonatal intensive care unit (NICU) admission have a known increased risk of refractive errors. While high-risk infants (e.g., ≤ 30 weeks gestation, syndromic) are universally screened by ophthalmology, moderately preterm infants and those with other neonatal illnesses may not receive adequate vision screening due to limited access to autorefraction equipment and trained staff. Objective: To achieve vision screening for refractive errors using a photo-refractometer (SPOT Vision Screener™) in 80% of eligible children aged 1-3 years attending the NICU follow-up clinic at least once per year by December 2025. Design/Methods: Baseline data from December 2024 visits identified eligible patients (ages 1-3 years with no ophthalmology follow-up) who had missed vision screening. Process, outcome, and balancing measures were defined (Fig. 1), and clinic staff were trained in device use. Eligible children without a vision screen in the past year were screened using the autorefractometer, with up to three attempts made per child. Abnormal results received referral to ophthalmology for confirmation and treatment. Screening results and follow-up outcomes were tracked in the electronic medical record (EMR). Results: At baseline, none of the eligible patients were screened. During PDSA cycle 1 (January-March), 100% (11/11) of eligible children were screened, with three abnormal results and one with confirmed refractive error and prescribed glasses. In PDSA cycle 2 (April-July), 13 of 15 eligible children (87%) were screened with four abnormal results and one confirmed refractive error and prescribed glasses. During Cycle 3 (August-October), 8 of 9 eligible children (89%) were screened, with two abnormal results pending evaluation. Screening rates improved significantly across cycles, with early identification and treatment initiated for confirmed cases.
Conclusion(s): Implementation of autorefractor-based vision screening in the NICU follow-up clinic improved screening rates and facilitated earlier detection of refractive errors in at risk toddlers. Ongoing challenges include delays in ophthalmology follow-up and limited data on amblyopia outcomes. Continued quality improvement efforts and strengthened referral pathways are essential to sustain progress and optimize health in this vulnerable population.
Figure 1: QI measures defined and Process map
Figure 2: Driver Diagram
Figure 3: Run chart of eligible patients who were screened during the PDSA cycles

 Credit")
.jpg "Majana Miller, DO, MHSA photo")