24 - The role of community health workers in integrated behavioral health
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3021.24
Phoebe Sloane, Brown University School of Public Health, Providence, RI, United States; Ruben G.. Martinez, The Warren Alpert Medical School of Brown University, NORTH PROVIDENCE, RI, United States; Radley C. Sheldrick, UMass Chan Medical School, Shrewsbury, MA, United States; Jessica E. Rosenberg, Boston Medical Center, Boston, MA, United States; Emily Feinberg, Hassenfeld Child Health Institute, Brown University School of Public Health, Providence, RI, United States; Charlotte Vieira, Boston Medical Center, Concord, MA, United States; Elijah E. Boliver, Boston Medical Center, Boston, MA, United States; Anita Morris, Boston Medical Center, Boston, MA, United States
PhD Student, Health Services Research Brown University School of Public Health Providence, Rhode Island, United States
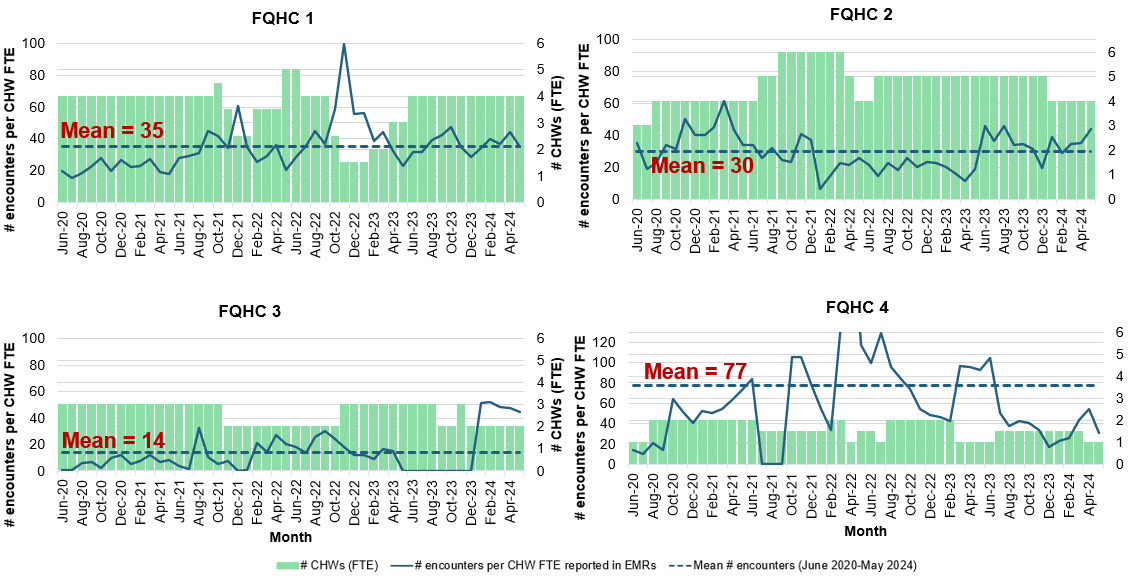
Background: Integrated behavioral health (IBH) models aim to improve access to behavioral health (BH) services through primary care. TEAM UP, a comprehensive pediatric IBH model for patients from birth to young adulthood, offers two innovations: multidisciplinary, team-based care and inclusion of community health workers (CHWs). Objective: This study examines: (a) diverse CHW roles in pediatric IBH, and (b) how pediatric practices tailor CHW roles to local needs. Design/Methods: TEAM UP was implemented at 4 federally qualified health centers (FQHCs) from 2020 to 2024. CHWs documented encounters in a standardized electronic health record (EHR) template. To estimate CHW productivity, we divided total encounters per month by total full-time equivalent (FTE) CHWs. EHR analyses examined service variation over time for two six-month periods (April-September 2022 & 2024) selected for data completeness and comparability. We checked results with member FQHCs in rapid qualitative interviews. Results: Of 42,415 children receiving IBH care at TEAM UP FQHCs, 8,192 had documented CHW encounters. Though staff estimated 80-120 encounters per CHW FTE per month, documented productivity was lower (Figure 1) with means of 14 (FQHC 3), 30 (FQHC 2), 35 (FQHC 1), and 77 (FQHC 4). Interviews revealed likely systematic undercounting of certain CHW encounters (e.g. outreach) and EHR data entry challenges.
CHWs documented numerous services to address material (e.g. food, housing) and behavioral health (e.g. service navigation) needs (Table 1). Services varied between (Table 1) and within FQHCs (Table 2). Member checks revealed reasons for variation. For example, FQHC 2 had case managers for material needs; thus, CHW encounters focused on BH, mainly navigation for school-based services (43.0%) and outpatient counseling (37.8%). At FQHCs without case managers, CHW encounters focused on material needs, mostly food (37.8% at FQHC 1, 40.1% at FQHC 3), followed by housing (28.5%) at FQHC 1 and other community resources (42.8%) at FQHC 3.
Within FQHCs, service provision changes reflect local needs and implementation learning (Table 2). For example, FQHC 3 CHW encounters shifted from BH needs (84.9% in 2022) to material needs (50.7% in 2024). FQHC 2 encounters remained focused on BH, increasing from 81.4% (2022) to 93.7% (2024).
Conclusion(s): Findings show diverse contributions of CHWs to IBH in pediatric primary care. Findings also reveal documentation challenges, demonstrating the need for operational support to ensure robust CHW documentation workflows. TEAM UP will discuss potential improvements in light of these results.
Figure 1. Pediatric practice variation in mean number of encounters per month per community health worker (CHW) full-time equivalent (FTE)
Table 1. Types of services provided by community health workers by pediatric practice
Table 2. Variation in types of service provided over time in two pediatric practices

.png)
.png)
