172 - Improving Outcomes for Patients Newly Diagnosed with Systemic Lupus Erythematosus
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3166.172
Melissa M. Hazen, Boston Children's Hospital, Boston, MA, United States; Esra Meidan, Boston Children's Hospital, Boston, MA, United States; Ankana Daga, Boston Children's Hospital, Boston, MA, United States; Maria Biancarelli, Boston Children's Hospital, SOUTH WALPOLE, MA, United States; Anthony Dekermanji, Boston Children's Hospital, Boston, MA, United States; Amy McDonough, Boston Children's Hospital, Braintree, MA, United States; Brittany Esty, Boston Children's Hospital, Boston, MA, United States; Caitlyn M. Dorsey, Boston Children's Hospital, Boston, MA, United States
Attending Physician Boston Children's Hospital Boston, Massachusetts, United States
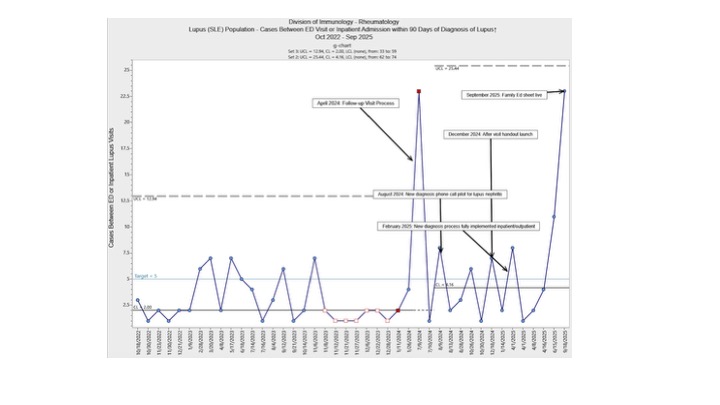
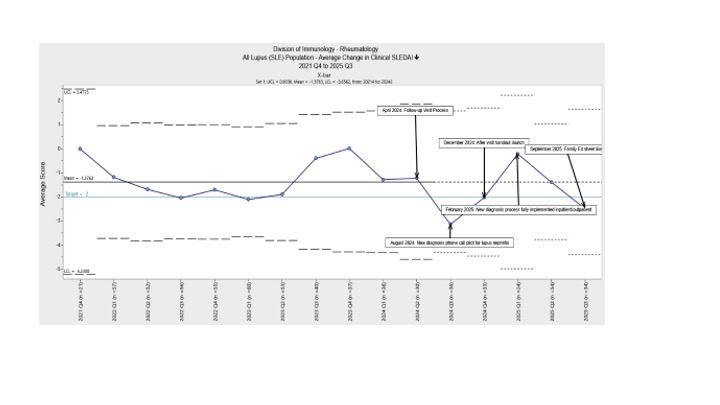
Background: SLE is an autoimmune disease with considerable morbidity and mortality. Given diverse manifestations, diagnosis may be delayed, leading to high disease burden at diagnosis. Onset may be rapid and severe, with advanced disease at diagnosis. New patients may not be familiar with SLE, which may lead to medication mistakes, care lapses and other avoidable errors. Thus, the period around SLE diagnosis can be one of high disease activity and intense resource utilization rendering it an ideal opportunity for interventions to improve care processes and disease-related outcomes. Objective: Global aim: We sought to improve care for patients newly diagnosed with SLE. SMART aims: (1) Increase the cases between an emergency department (ED) visit or admission for new patients from 2 to 5 by June 2025. (2) Decrease the average SLEDAI score change for all patients from -0.65 to -2 by June 2025. Design/Methods: Using the Model for Improvement, we outlined care barriers on a fishbone diagram and used a process map to understand communication flow after diagnosis. After prioritizing interventions with an impact effort matrix, we developed a process for new patients. The rheumatology nurse (RN), social worker (SW), and administrative team are notified at diagnosis. Patients/families are provided with verbal and written education about SLE and care needs, like medications and follow up. The SW visits the family and assesses for HRSN. Before discharge, the next 3 rheumatology appointments are scheduled. At discharge, material about how/when to seek care is provided. Within 1 week of discharge, the RN calls to address questions that arise. If clinically indicated, sooner follow up is scheduled. We developed a swim lane diagram to outline the new process with all stakeholders (Fig 1). We used statistical process control charts to assess results. Results: After our interventions, cases between an ED visit or admission for new patients demonstrated special cause variation with an increase from a baseline of 2 cases to an average of 4.16 cases, with the most recent data point being at 22 cases (Fig 2). The average change in clinical SLEDAI for the entire SLE population remained stable (Fig 3).
Conclusion(s): Our care package has led to measurable improvements in outcomes for patients newly diagnosed with SLE, particularly in preventing ED visits and admissions. With time, we hope to improve change in SLEDAI scores. We will continue to refine this process through PDSA cycles to further improve the care delivered to this high-risk population.
Figure 1. Swimlane Diagrams of Ideal State Process from Inpatient and Outpatient Settings Slide1.jpeg
Figure 2. Interventions Lead to Increased Cases between ED Visits or Admissions for Patients Newly Diagnosed with SLE
Figure 3. Average Change in Clinical SLEDAI Remains Stable Over Baseline and Intervention Period

 Credit")
 photo")