559 - From Rules to Learning: Deep Learning–Based CTG Waveform Analysis Outperforms ACOG Category III in Predicting Risk of Perinatal Depression
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3540.559
Vivek V. Shukla, University of Alabama at Birmingham, Birmingham, AL, United States; Avinash Singh, Children's of Alabama, Birmingham, AL, United States; Manasa Kalidindi, University of Alabama School of Medicine, Birmingham, AL, United States; yumo Xue, UAB, Birmingham, AL, United States; Kevin S. Shrestha, University of Alabama School of Medicine, Birmingham, AL, United States; Victoria C. Jauk, University of Alabama School of Medicine, Birmingham, AL, United States; Dhong-Jin Kim, University of Alabama School of Medicine, Birmingham, AL, United States; Lynda Ugwu, University of Alabama at Birmingham School of Medicine, Birmingham, AL, United States; Alan Tita, University of Alabama at Birmingham, Birmingham, AL, United States; Waldemar Carlo, University of Alabama, Birmingham, AL, United States; Namasivayam Ambalavanan, University of Alabama School of Medicine, Birmingham, AL, United States; Arie Nakhmani, University of Alabama at Birmingham, Birmingham, AL, United States; Akila Subramaniam, University of Alabama School of Medicine, Birmingham, AL, United States
Assistant Professor University of Alabama at Birmingham Birmingham, Alabama, United States
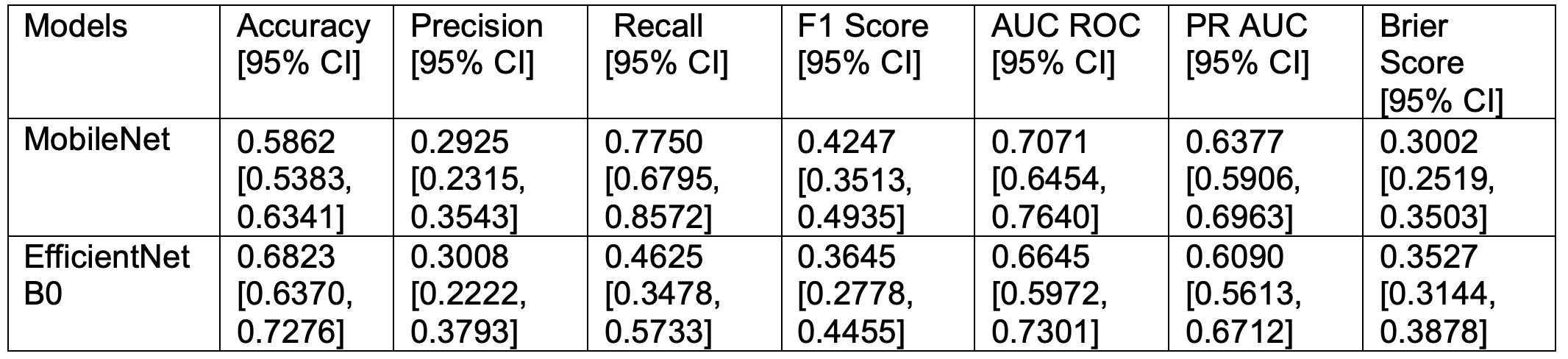
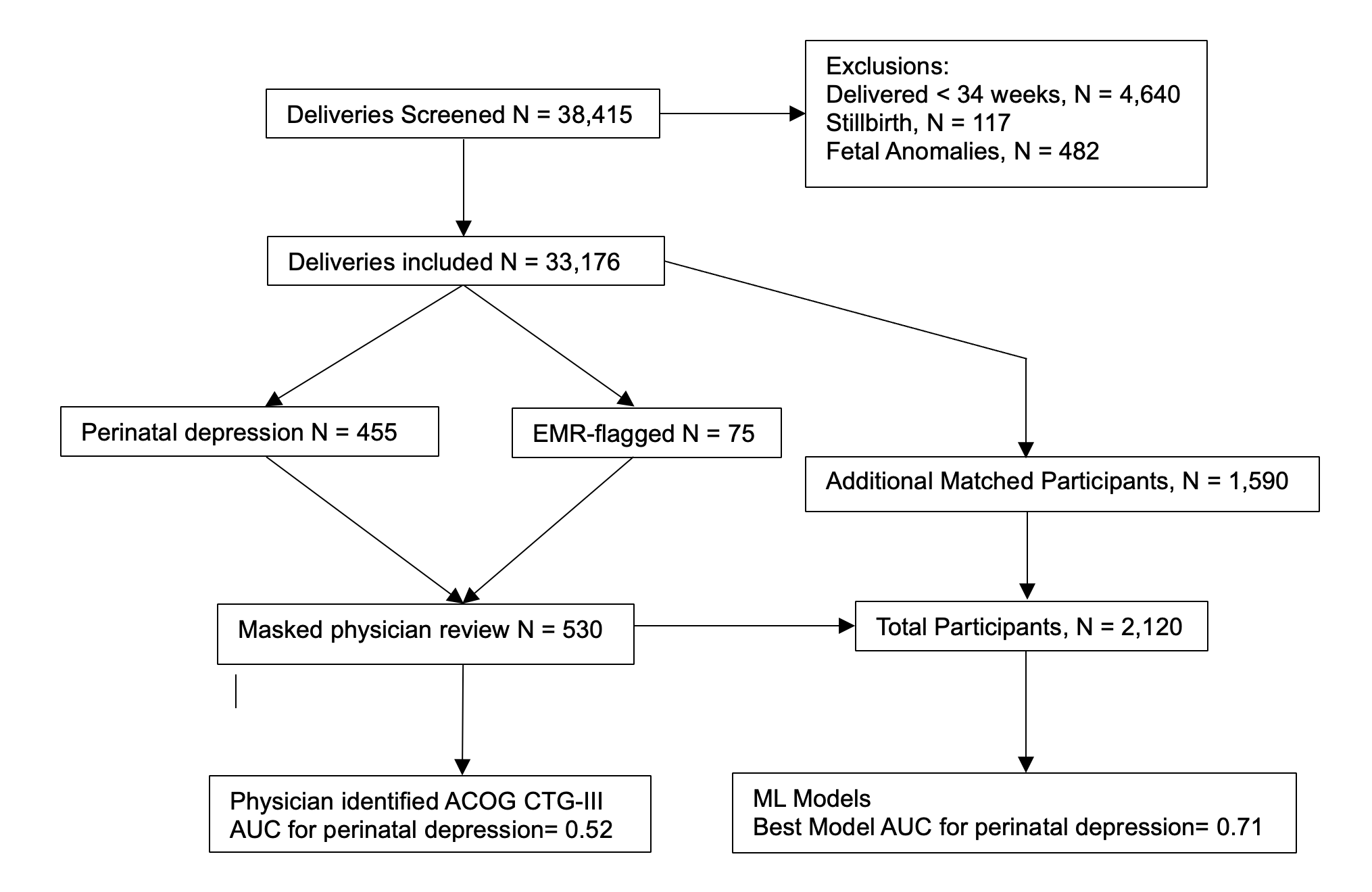
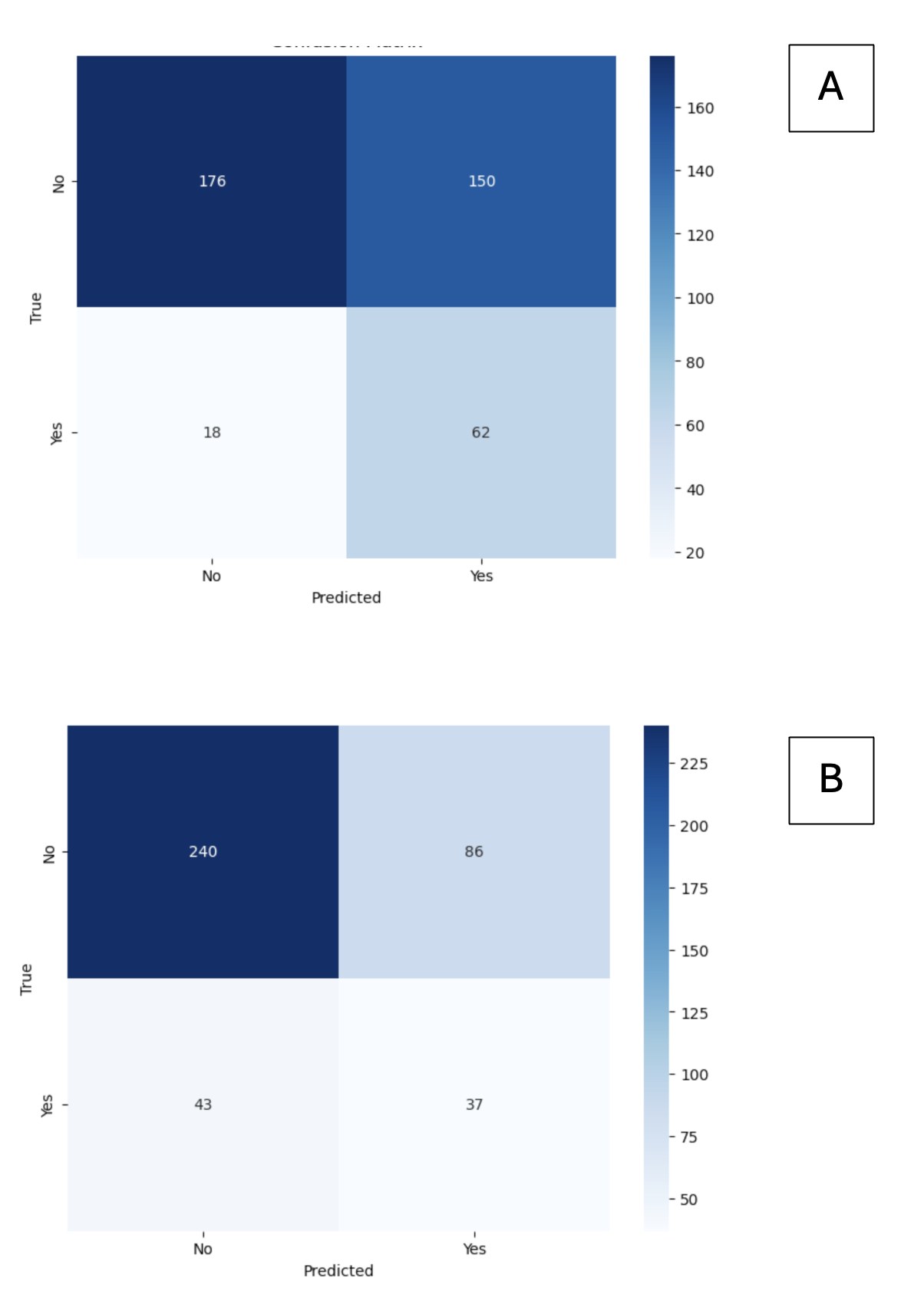
Background: Cardiotocography (CTG) is routinely used for intrapartum fetal monitoring. However, ACOG Category III classification demonstrates limited predictive ability for identifying fetuses at risk of perinatal depression (PD, defined as fetal acidemia-cord pH ≤7.0 and base deficit ≥16 mmol/L, and a 5-minute Apgar score < 5). Objective: To test the hypothesis that deep learning-based analyses of CTG waveforms would improve PD risk prediction compared with ACOG Category III interpretation. Design/Methods: We included singleton live births ≥34 weeks' gestation delivered at the University of Alabama at Birmingham from January 1, 2013, to December 31, 2023, excluding those with major structural or chromosomal anomalies. Category III CTG was defined per ACOG criteria as absent variability with bradycardia, recurrent late or variable decelerations, or sinusoidal pattern. A two-step process was used to identify CTG categories: an EMR query flagged tracings with ≥2 late/variable decelerations in 30 minutes during CTG monitoring, and all neonates with PD were added, followed by masked physician review by a Maternal-Fetal Medicine fellow. Controls (3:1) were matched by gestational age and delivery date. Fetal heart rate (FHR) waveforms from the final hour before delivery were processed, converted to images, and analyzed with deep learning models (MobileNet and EfficientNetB0) using a 60/20/20 (train/validation/test) patient-level split. Accuracy, F1, AUC ROC, PR AUC, and Brier scores were assessed with 95% bootstrapped CIs. Results: Of 38,415 deliveries screened, 33,176 were included in the study. Among 455 infants with PD, 15 (3%) had ACOG-defined Category III CTG, yielding a sensitivity of 3% (AUC ROC = 0.52) and correctly identifying ~3 of every 100 PD infants. In contrast, deep-learning analysis of CTG waveforms from 2,120 participants (455 with PD, 75 EMR-flagged, and 1590 matched controls; Figure 1) demonstrated better performance: The MobileNet model achieved the best performance (AUC ROC = 0.71, recall = 0.77, precision = 0.29, F1 = 0.42, Brier = 0.30), correctly identifying ~77 of every 100 PD infants, ~74 more than Category III CTG. EfficientNetB0 (AUC ROC = 0.66) showed lower but better than Category III CTG performance (Table 1, Figure 2)
Conclusion(s): Machine-learning analysis of intrapartum CTG showed better performance for predicting perinatal depression versus ACOG Category III CTG classification. These results support further validation to develop clinically useful risk identification tools.
Table 1: Model Performance Comparisons
Figure 1: Participant Flow Diagram
Figure 2: Confusion Matrices for A) MobileNet and B) EfficientNetB0 Models.

.jpeg.jpg "Vivek V. Shukla, MD (he/him/his) photo")