Session: Neonatal General 7: Cardiology and Hemodynamics
431 - Development of a Real-Time Early Prediction System for Metabolic Acidosis Using Vital Sign Monitoring in High-Risk Premature Infant
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3416.431
Jeong Eun Shin, Yonsei University College of Medicine, Seoul, Seoul-t'ukpyolsi, Republic of Korea; Sungbo Shim, Yonsei medical school, Seoul, Seoul-t'ukpyolsi, Republic of Korea; Ju Hyun Jin, Yonsei College of Medicine, Seoul, Seoul-t'ukpyolsi, Republic of Korea; Soon Min Lee, Yonsei University College of Medicine, Seoul, Seoul-t'ukpyolsi, Republic of Korea; Seng Chan You, Yonsei University College of Medicine, Seoul, Seoul-t'ukpyolsi, Republic of Korea; Sojin Yoon, Yonsei university College of medicine, Gangnam-gu, Seoul-t'ukpyolsi, Republic of Korea
Associate Professor Yonsei University College of Medicine Yonsei University College of Medicine Seoul, Seoul-t'ukpyolsi, Republic of Korea
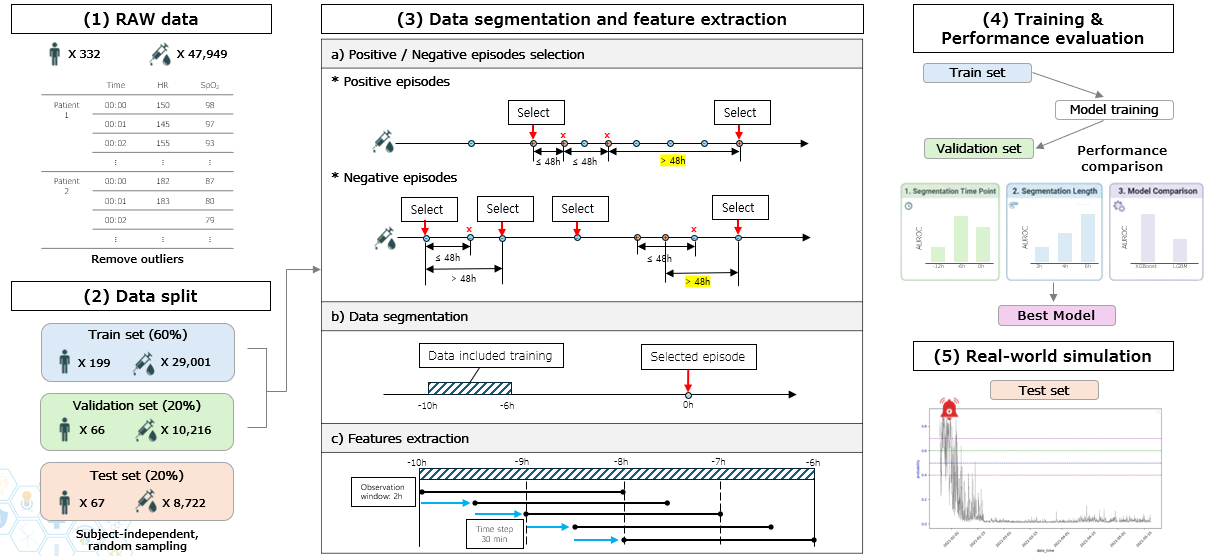
Background: Preterm infants are highly vulnerable to systemic illnesses, often preceded by metabolic acidosis. Metabolic acidosis can be detected by blood gas analysis before clinical signs and serves as a marker of deterioration. However, repeated blood sampling is invasive and may cause blood loss. A non-invasive prediction tool using routinely monitored continuous vital signs could provide timely alerts and improve safety. Objective: We aimed to develop a machine-learning model using continuous vital signs to predict metabolic acidosis in preterm infants and assess its clinical utility through real-time simulation. Design/Methods: We retrospectively included 322 preterm infants with birth weight < 1500 g or gestational age < 32 weeks, admitted to the NICU of Severance Children's Hospital between July 2020 and November 2024. Heart rate and respiratory rate, sampled at one-minute intervals, were linked to blood gas results from the i-STAT analyzer (Abbott, MN). Metabolic acidosis was defined as pH < 7.2 and base excess <−7 mmol/L. From 4-hour segments of vital signs, 129 features including statistical and temporal -features were extracted. Outliers were removed and data split into training, validation, and test sets. XGBoost models were trained at three time points from the time of blood gas analysis (−4 to 0h, −12 to −6h, −16 to −12h). Performance was assessed by AUROC, PRAUC, F1, accuracy, PPV, NPV, sensitivity, and specificity. Results: Mean gestational age was 29.2 ± 3.1 weeks and birth weight 1175 ± 497 g. The model using data segments from 6 hours before the event (-10 h to -6 h) showed the best overall performance, with an F1 score of 0.206, weighted F1 of 0.949, accuracy 92.2%, PPV 11.8%, and specificity 92.3%. Although the model trained with data immediately before the episode (-4 h to 0 h) achieved the highest AUROC (0.943) and AUPRC (0.169), the 6-hour model was selected for its balanced performance under class imbalance. In continuous real-time prediction, it achieved sensitivity 80.5-91.4%, specificity 81.5-88.8%, PPV 9.3-13.0%, and NPV 99.5-99.8%.
Conclusion(s): A machine-learning algorithm using continuous vital signs offers a non-invasive bedside monitoring tool. By providing early warnings of deterioration, it supports decision-making, reduces blood tests, and promotes baby-friendly care. Reliable exclusion of acidosis may reduce unnecessary sampling, while early prediction enables timely evaluation for sepsis or NEC. External validation in larger prospective cohorts is required to confirm generalizability and clinical utility.