Session: Neonatal Hemodynamics and Cardiovascular Medicine 2
470 - Acetaminophen Serum Levels and Closure of Patent Ductus Arteriosus in Infants Born at 22 to 25 Weeks Gestation
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3455.470
Saswat K Jha, USA Health Children and Women Hospital, Mobile, AL, United States; Michael Zayek, University of South Alabama Children's and Women's Hospital, Mobile, AL, United States; Fabien Eyal, University of South Alabama College of Medicine, Mobile, AL, United States; Cristina E. Gavrilita, University of South Alabama Children's and Women's Hospital, Mobile, AL, United States; Bianca M. Vamesu, University of South Alabama Children's and Women's Hospital, Mobile, AL, United States
USA Health Children and Women Hospital Mobile, Alabama, United States
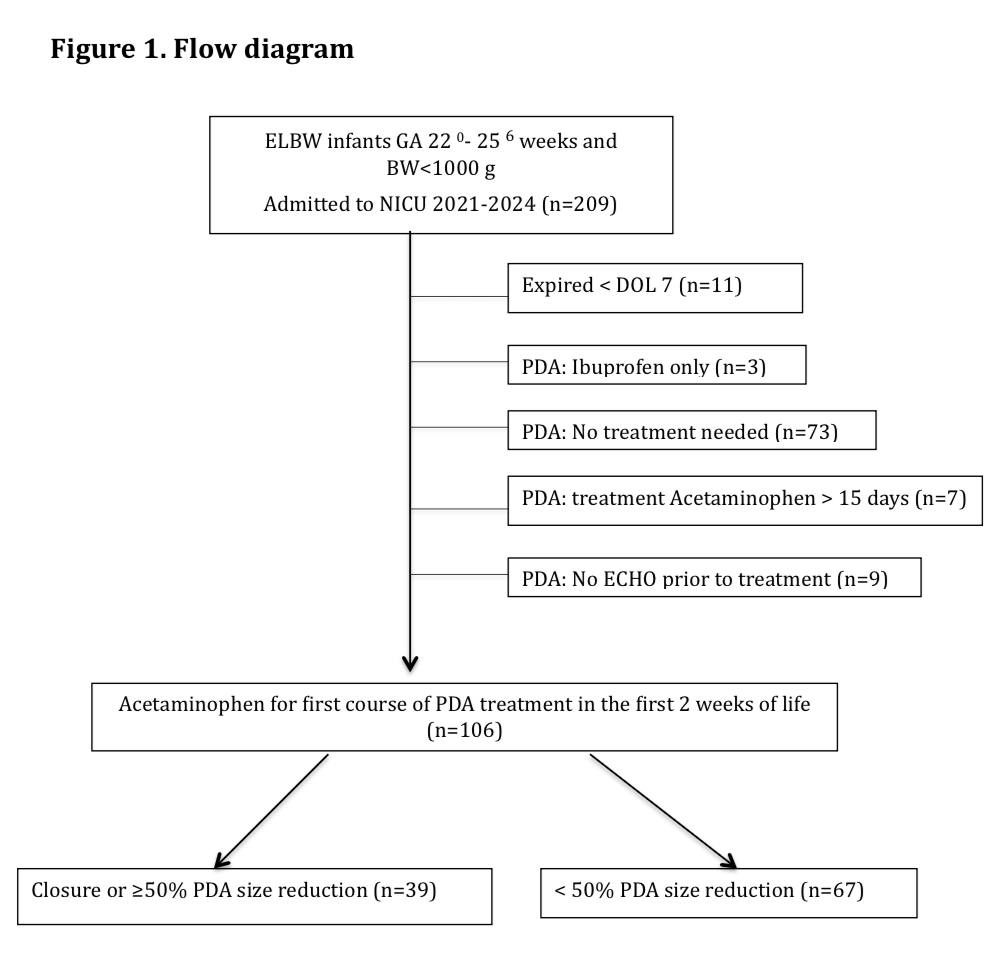
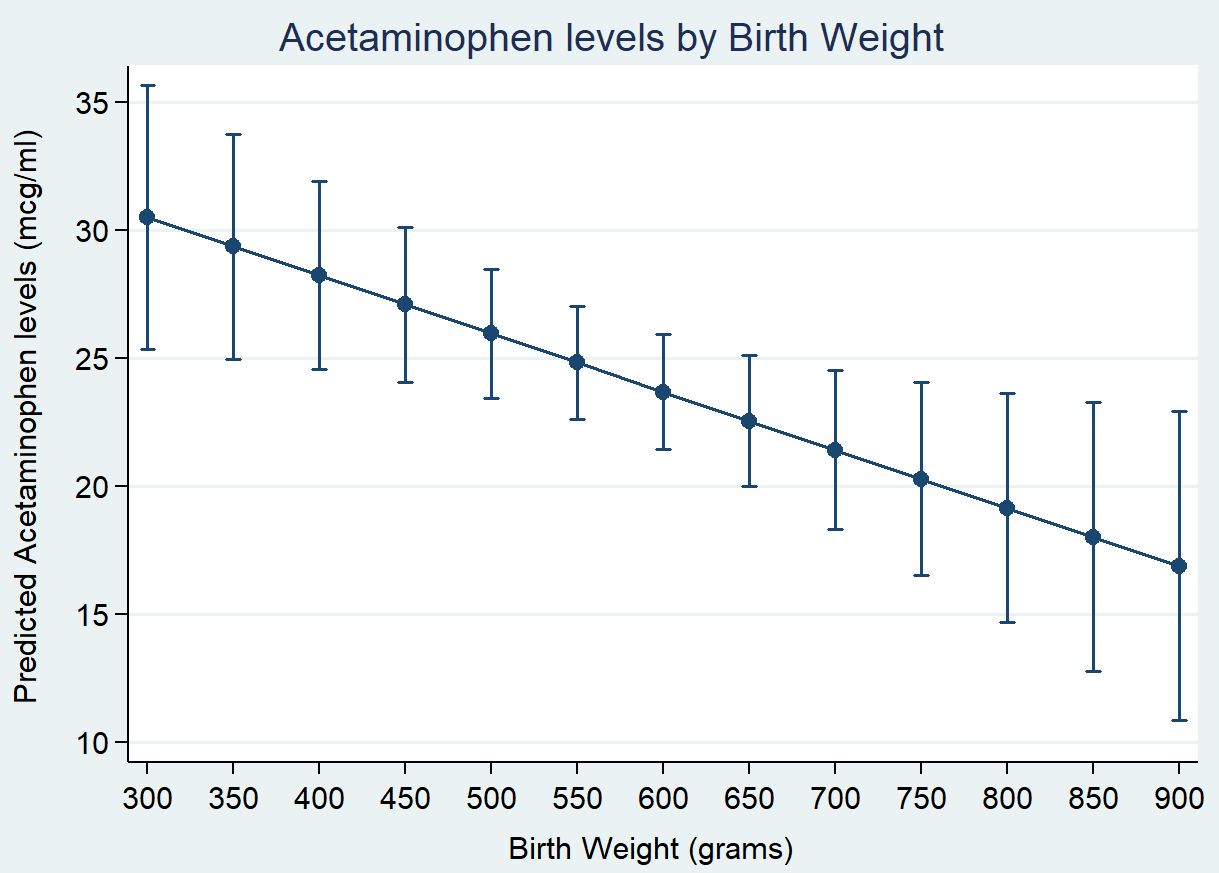
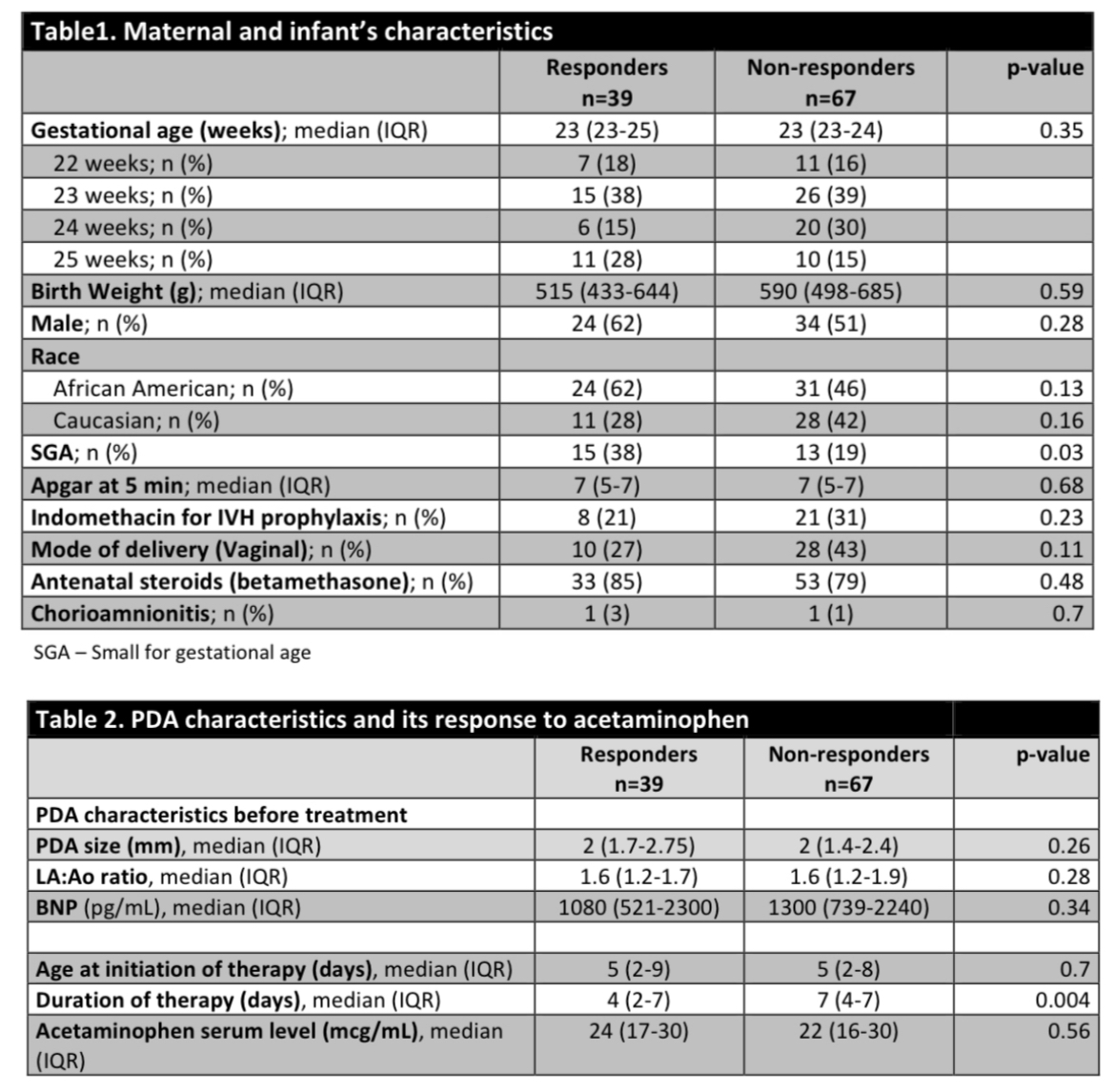
Background: Acetaminophen is widely used as a first-line treatment for PDA in extremely preterm infants due to its favorable safety profile compared with indomethacin and ibuprofen. However, data linking treatment response to the serum acetaminophen levels in this population remain limited. Objective: To determine whether higher serum acetaminophen levels are associated with increased rates of PDA closure in infants < 26 weeks gestation. Design/Methods: We retrospectively reviewed the charts of infants born at 22 to 25 weeks' gestation who were admitted to a single level III NICU between January 2021 and December 2024 and were treated with acetaminophen for hemodynamically significant PDA within the first 15 days of life (n=209). Infants who died within the first week of life, did not require PDA treatment, or received ibuprofen as first-line therapy were excluded (n=103) (Fig 1). All included infants received acetaminophen 15 mg/Kg every 6 hours for 3 to 7 days. On day 3 of therapy, serum acetaminophen and BNP levels were obtained, and PDA size was reassessed by echocardiography. Treatment was discontinued after 8 doses if PDA closure occurred or if serum acetaminophen concentration exceeded 30 mcg/mL. Infants were classified as responders (PDA closure or ≥ 50% size reduction after the first course)(n=39) and non-responders(n=67). Potential predictors, including serum acetaminophen levels, were compared between the two groups and a multivariable logistic regression was used to identify independent predictors of response. IRB approval was obtained. Results: Acetaminophen treatment was initiated in 106 infants at a median age of 5 days, with similar distribution in both responders (IQR 2-9) and non-responders (IQR 2-8). Response rates (PDA closure or >50% reduction in diameter) did not differ across serum acetaminophen levels: 28% at < 20 mcg/mL, 43.6% at 20-30 mcg/mL, and 39.3% at levels > 30 mcg/mL (p=0.352). Although lower birth weight was associated with higher serum acetaminophen levels, gestational age, gender, race, baseline PDA size, birth weight and serum acetaminophen levels were not associated with treatment response (Fig.2). Among all variables, only being small for gestational age was independently associated with improved response, 38% vs. 19%, OR of 2.7 (95% CI: 1.1-6.9), p = 0.04. (Tables 1, 2)
Conclusion(s): Ductal response to acetaminophen in infants born at 22 to 25 weeks of gestation was not associated with serum acetaminophen levels. Ongoing data collection will evaluate whether prematurity-related complications may affect PDA closure.
Flow Diagram
Acetaminophen Levels by birth Weight
Table 1: Maternal and Infants characteristics, Table 2: PDA characteristics and its response to acetaminophen.