114 - Does real-time Point-of-Care Ultrasound(POCUS) for neonatal Peripherally Inserted Central Catheter(nPICC) tip confirmation in NICU reduces the Catheter Line Associated Blood Stream Infection (CLABSI)?
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3109.114
RASHIDA JAVED, University Hospitals Birmingham NHS Trust, LEICESTER, England, United Kingdom; Kanwal Mahadev, Leicester university Hospital NHS trust, Leicester, England, United Kingdom; Victoria Collis, Birmingham Heartlands Hospital, Birmingham, England, United Kingdom; Dhanwanti Dhanwanti, Other, Manchester, England, United Kingdom; Pri Madawala, University, Birmingham, England, United Kingdom; Mona Noureldein, University Hospitals Birmingham, Birmingham, England, United Kingdom; Harsha Gowda, University Hospitals Birmingham NHS Trust, Birmingham, England, United Kingdom
University Hospitals Birmingham NHS Trust LEICESTER, England, United Kingdom
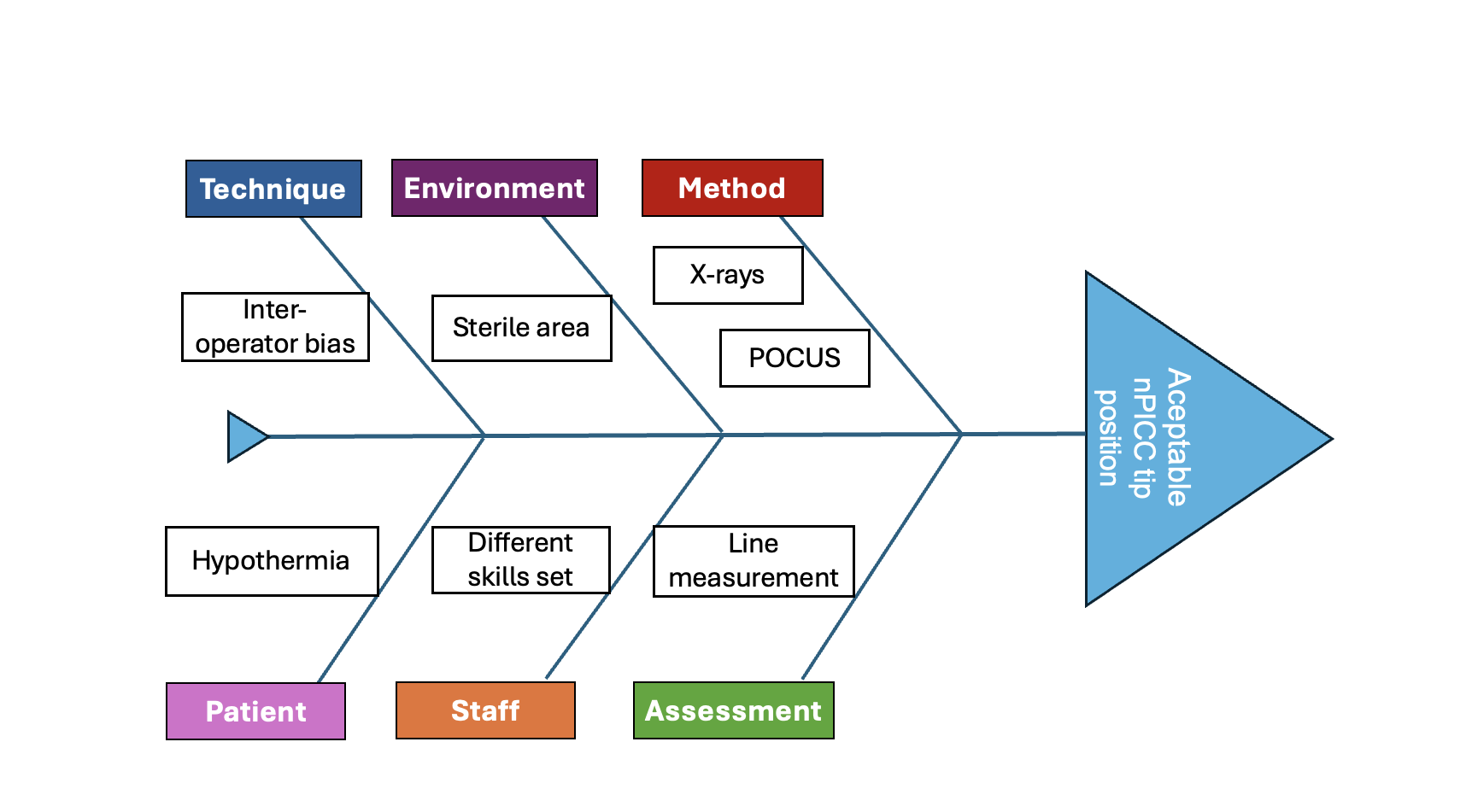
Background: Point-of-care ultrasound (POCUS) is an emerging diagnostic and procedural tool in the Neonatal Intensive Care Unit (NICU). POCUS allows the clinicians for non-invasive, feasible and cost-efficient intervention which makes it a favourable investigation on the NICU. The placement of neonatal Peripherally Inserted Central Catheter (nPICC) is a common procedure but one that does not come without inherent risk. POCUS is becoming more widely used to assess the catheter tip position. Malpositioned nPICCs can lead to multiple adjustments which can increase the risk of Catheter Line Associated Blood Stream Infection (CLABSI). Objective: This Quality Improvement Project (QIP) aims to reduce number of repositions and rate of CLABSI by using POCUS. Design/Methods: Step-1: Literature review Step-2: Retrospective data analysis on number of X-rays and nPICC adjustments (October 2021 - April 2022) We identified challenges such as methodological preferences between X-rays and POCUS, environmental factors such as maintaining a sterile field and risk of hypothermia in extreme preterm infants. Additional challenges were inter-operator bias and lack of POCUS trained clinician. Figure 1 Step-3: Implementation of real-time POCUS to confirm nPICC tip position (May 2022) Step-4: Prospective data collection on nPICC malpositions, adjustments and CLABSI (May 2022 - April 2024)
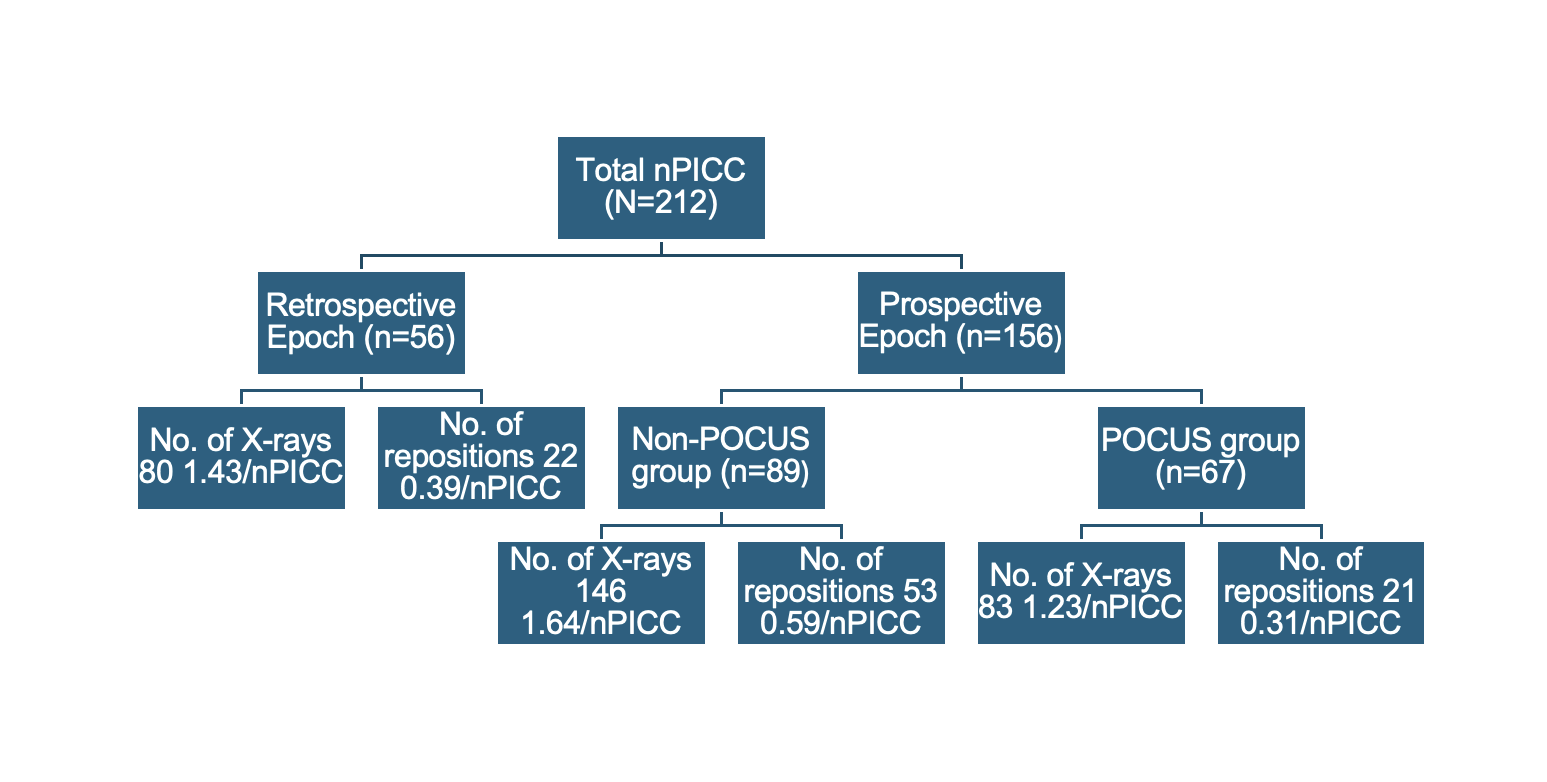
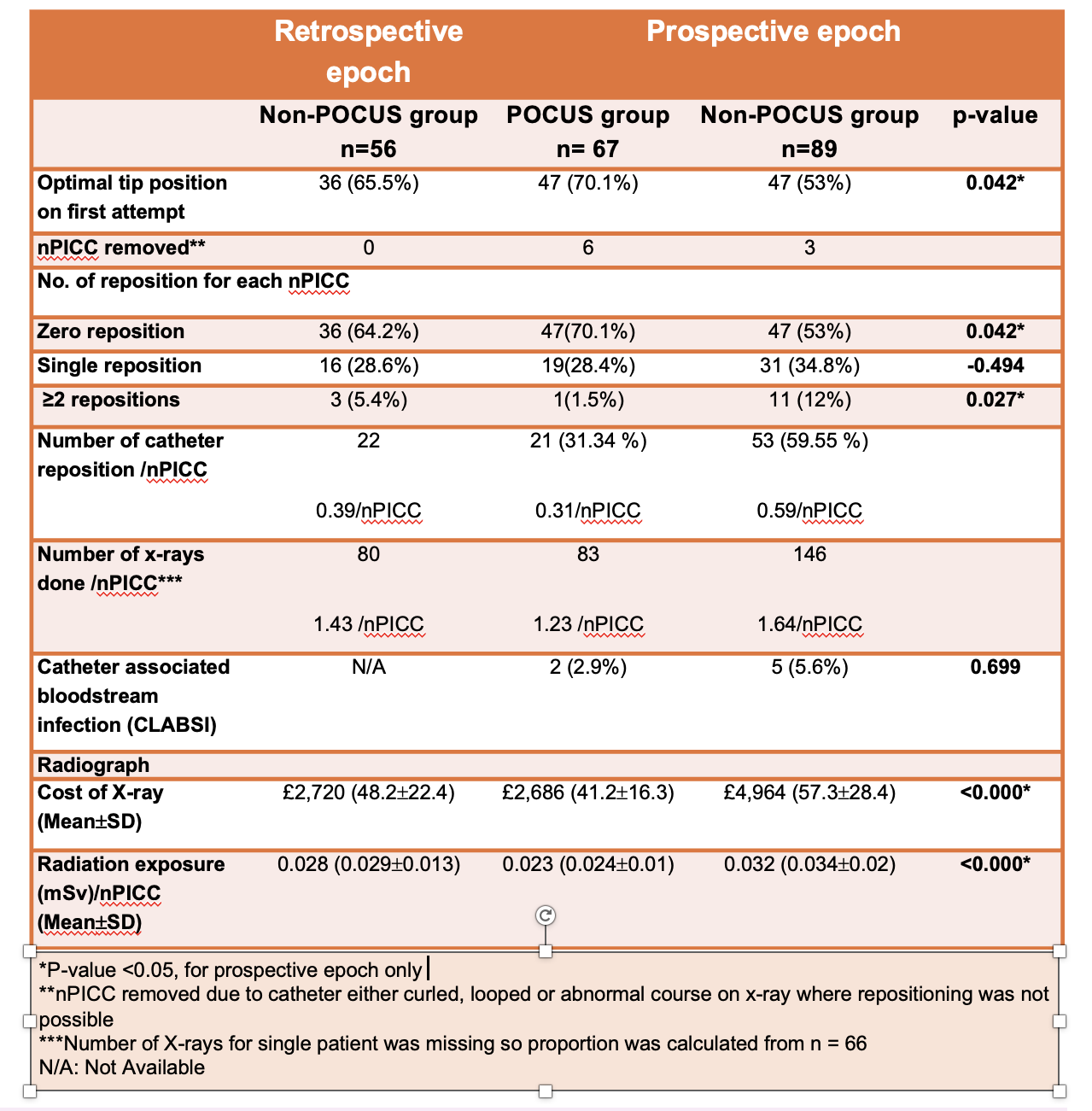
In step 4, X-ray was done after the real-time POCUS to check the final nPICC tip position. This is as per current national recommendation from BAPM (British Association of Perinatal Medicine). Results: Total of 212 nPICCs were analysed. Figure 2 Gestational age ranged from 22+6 to 39+4 weeks and birth weight from 410g to 3110g. With POCUS use, 82% of the nPICC needed only one X-ray to confirm the position compared with 51% in non-POCUS group. Whereas 70% of nPICC insertion required no adjustments in POCUS group compared to 53% in non-POCUS group. There was a reduction in the number of X-rays from 1.64/nPICC to 1.23/nPICC following POCUS implementation. CLABSI in POCUS group was 2.9%(2/67) compared to 5.6%(5/89) in non-POCUS group (p=0.699). Figure 3
Conclusion(s): Introduction of real-time POCUS to confirm nPICC tip position in NICU significantly reduced number of malpositions and catheter adjustments. Real-time POCUS during nPICC insertion can support more accurate tip placement on the first attempt. This results in lowering the number of catheter tip repositions, potentially reducing the risk of infection. There was a reduction in CLABSI in POCUS group, but it was not statistically significant due to small number of patients with catheter infection.
Fish bone diagram
Consort flow diagram
Comparison of results of POCUS and non-POCUS group