14 - Restraint use in the Emergency Departments of Hospitals in the Michigan Child Health Equity Collaborative (MI-CHEC) by Patient Characteristics
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3013.14
Susan Woolford, University of Michigan Medical School, Ann Arbor, MI, United States; Cheyney Dobson, University of Michigan Medical School, Ann Arbor, MI, United States; Miao Yu, University of Michigan, Ann Arbor, MI, United States; Harlan McCaffery, University of Michigan Medical School, Ann Arbor, MI, United States; Niko Kaciroti, University of Michigan Medical School, Ann Arbor, MI, United States; Patricia Andreski, University of Michigan Medical School, Ann Arbor, MI, United States; William E. Gillespie, University of Michigan Medical School, Ann Arbor, MI, United States; Brittany Bogan, C.S. Mott Children's Hospital, Ann Arbor, MI, United States; Deborah Niedbala, Children's Hospital of Michigan, Detroit, MI, United States; Adam M. Nicholson, Corewell Health Helen DeVos Children's Hospital, Byron Center, MI, United States; Gary Freed, University of Michigan Medical School, Ann Arbor, MI, United States
Associate Professor University of Michigan Medical School Ann Arbor, Michigan, United States
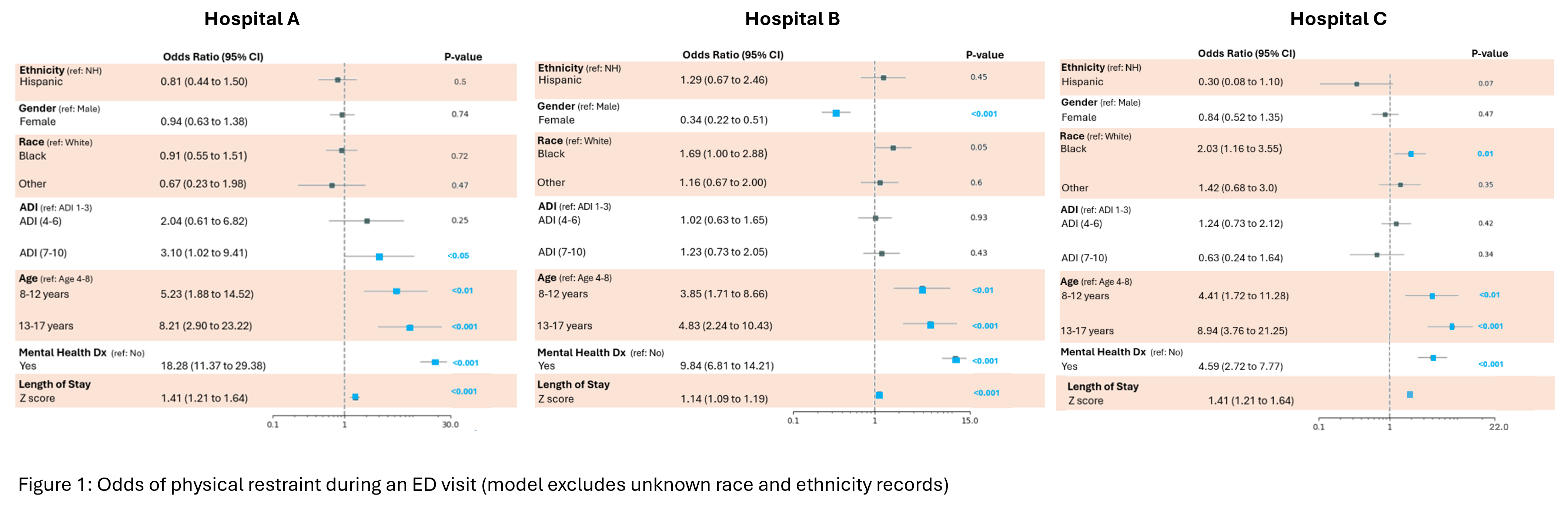
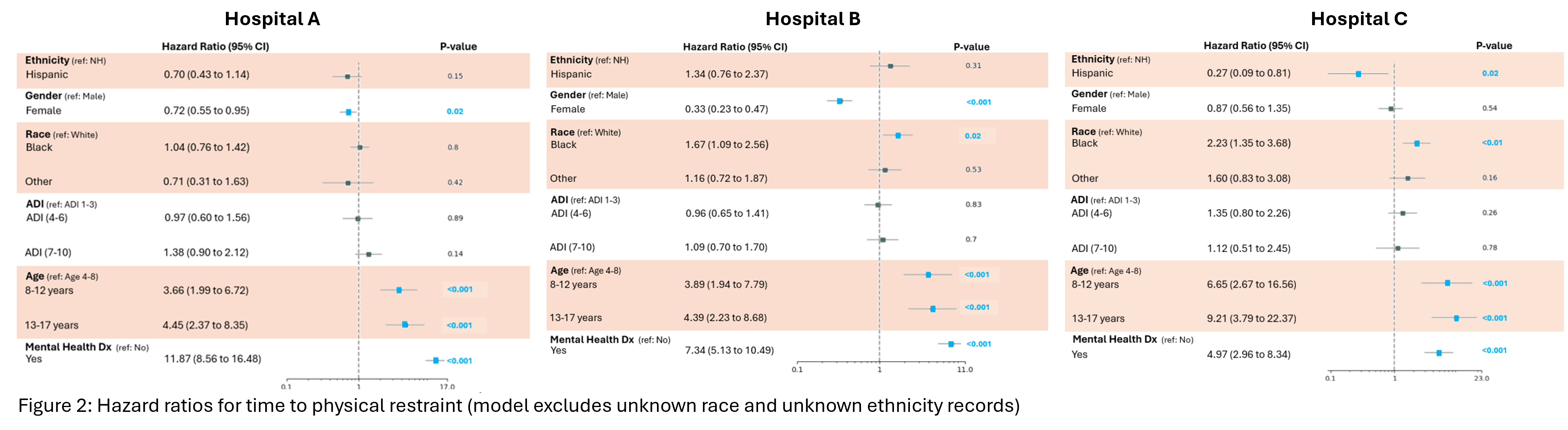
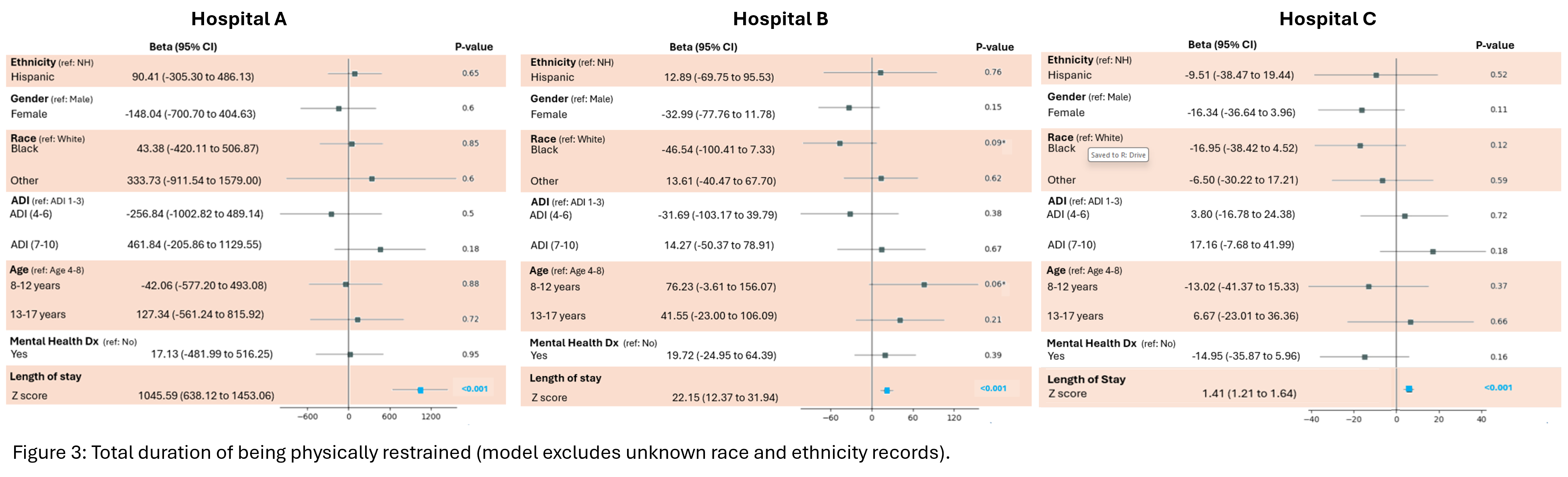
Background: Patient agitation in pediatric emergency departments (PED) can impede care and cause harm. To provide quality care and promote safety, managing agitation through physical restraint (PR) may be necessary. However, given known risks associated with the use of PR, it is important to ensure it is used appropriately and without bias. Little is known about whether PR is used differentially by patient characteristics in PEDs. Objective: To inform future improvement efforts, the objective of this study is to examine whether, in the 3 large Midwestern children's hospitals participating in the MICHEC Collaborative, PR use varies by key patient characteristics. Design/Methods: For this retrospective secondary data analysis, data were extracted from the electronic medical records (EMR) of the 3 MICHEC hospitals. The study population included encounters for patients (4 - < 18 years old) presenting to the ED from January 1, 2022 to July 31, 2024 (n=202,152). Rates of PR (as documented in the nursing flowsheets) were calculated. Associations between patient characteristics (i.e., race, ethnicity, socioeconomic status (SES) (assessed by Area Deprivation Index as a proxy), sex, age, and presence of a mental health diagnosis) and a) odds of PR, b) time to PR, and c) duration in PR were examined using logistic regression, Cox regression and linear regression respectively controlling for length of stay (LOS) as appropriate. Generalized Estimating Equations were used to account for repeat encounters during the study period. Results: Across the 3 hospitals, older age and the presence of a mental health diagnosis were associated with greater odds of PR (Fig 1) and these patients had a higher risk of PR sooner (Fig 2). Female patients had lower odds of PR and were restrained later after arrival at the ED in general (though this was only statistically significant at 2 hospitals). For race, ethnicity and SES, findings were not consistent. For example, Black patients had higher odds of PR at one hospital, a greater risk of PR sooner at another, and no differences in PR compared to White patients at the third. At a single hospital serving a larger population of patients from lower SES families, lower SES was associated with greater odds of PR. No meaningful differences in PR duration were noted (Fig 3).
Conclusion(s): Overall, PRs are used infrequently at the MICHEC PEDs. Higher odds of PR use for older patients and those with mental health diagnoses may be anticipated due to concerns for patient and staff safety. The findings revealed setting specific differences in PR use by race and SES that may warrant improvement efforts.
Figure 1: Odds of Physical Restraint in the Pediatric Emergency Department
Figure 2: Hazard Ratios for Time to Physical Restraint
Figure 3: Total Duration of Being Physically Restrained