697 - Emergency Department Return Rates for Pediatric Patients with Positive Sepsis Screening at Index Visit
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3674.697
Sarah Allen, Nationwide Children's Hospital, Columbus, OH, United States; Julia Lloyd, Nationwide Children's Hospital, Columbus, OH, United States; Sara Helwig, Nationwide Children's Hospital, Columbus, OH, United States
Pediatric Emergency Medicine Fellow Nationwide Children's Hospital Columbus, Ohio, United States
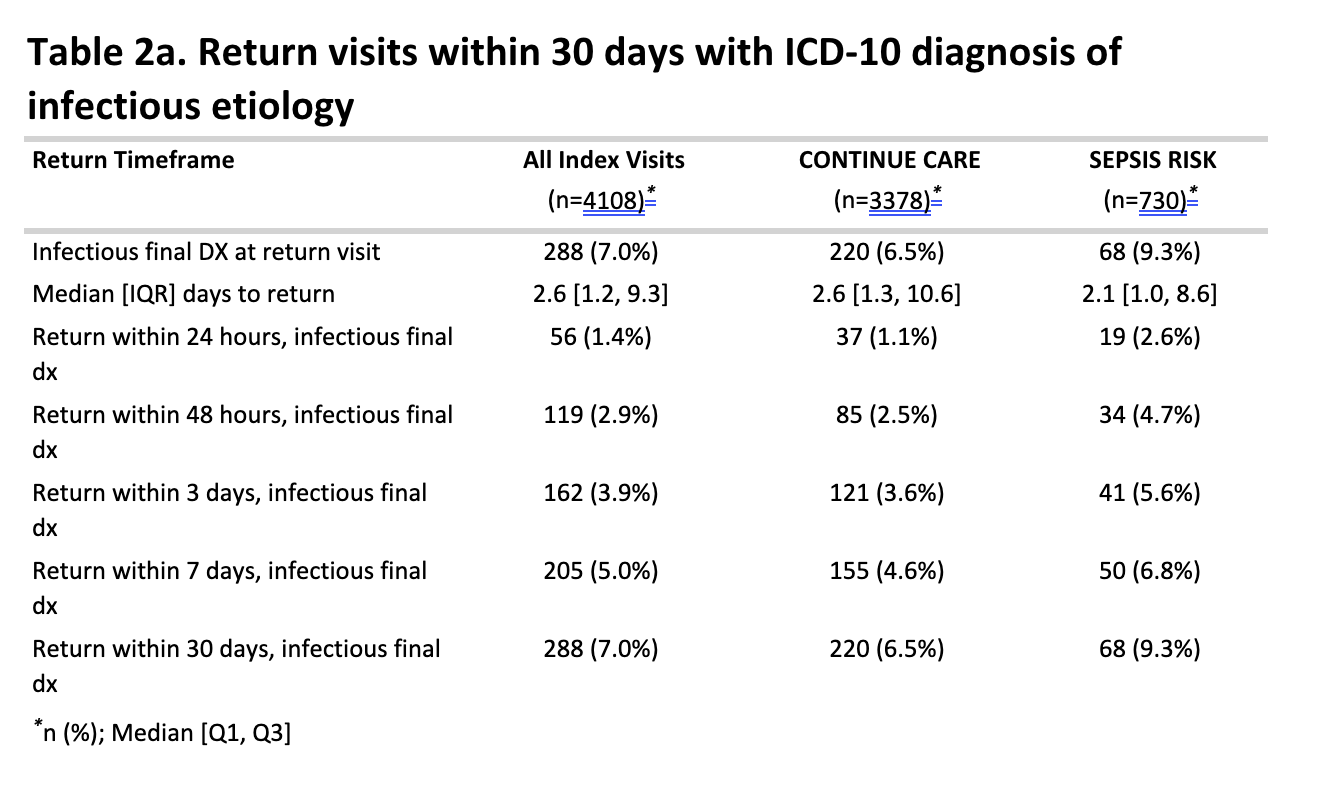
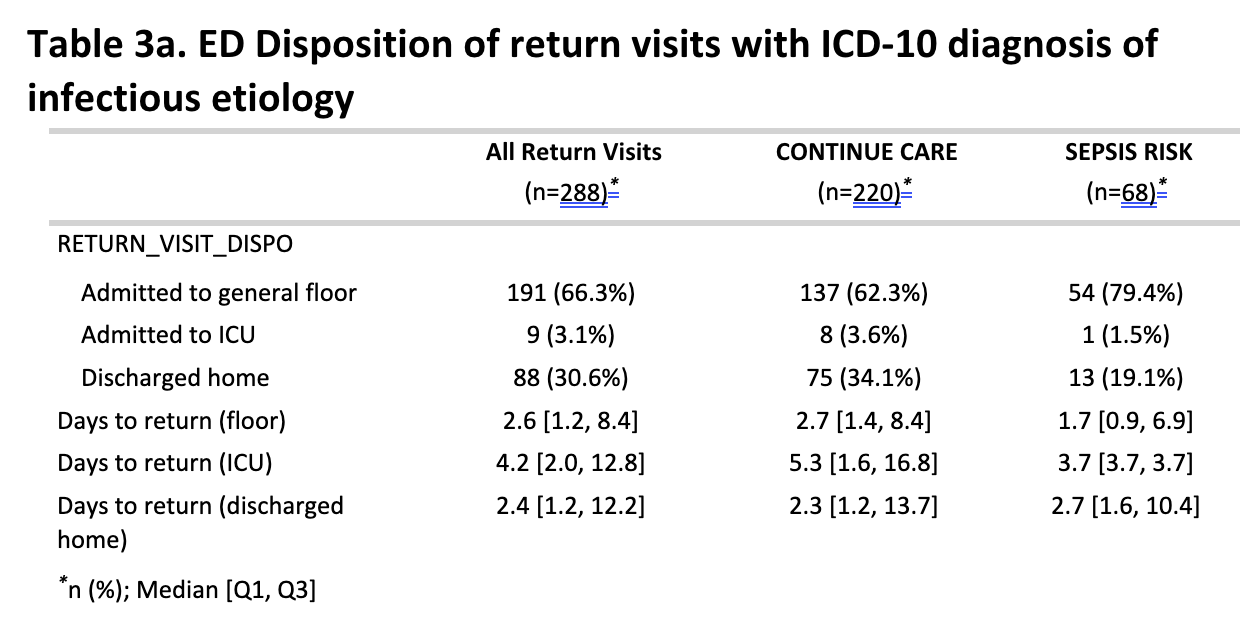
Background: Sepsis remains a significant cause of morbidity and mortality among pediatric patients. While readmission rates for children hospitalized with sepsis are well described, little is known about those who screen positive for sepsis in the Emergency Department (ED) but are discharged home. No previous studies have evaluated if these patients re-present at a higher rate than those without sepsis risk. Objective: The objective of this study was to determine the association between increased sepsis risk and the likelihood of an infectious return visit within 30 days among patients discharged home from the ED. Secondary aims included describing the timing and disposition of return visits by initial sepsis risk Best Practice Advisory (SRBPA) outcomes. Design/Methods: This retrospective cohort study included ED encounters from 2018-2023 at a free-standing quaternary care children's hospital in which an SRBPA fired and the patient was discharged home. An SRBPA fires when vitals and RN assessment reach a predetermined threshold, then an assessment is conducted by a physician to determine sepsis risk. Return visits, reason (identified by ICD-10 diagnostic codes) and timing, ED management, and disposition on return were compared across SRBPA outcomes. Results: Among 4108 patients with an SRBPA fire at their index visit to the ED and discharged home, 730 (17.8%) patients were deemed at risk for sepsis. Within 30 days, 288 (7.0%) patients returned to the ED with an infectious diagnosis (median 2.6 days); 68 (23.6%) of these occurred in patients initially identified as at risk of sepsis. Return rates were higher among at-risk patients (9.3%) compared with those not at risk (6.5%). Of the 288 patients who returned, 39 (13.5%) had an SRBPA fire at return visit, with 13 (4.5%) again characterized as at risk for sepsis. At return, 191 (66.3%) were admitted to a pediatric floor, 9 (3.1%) required ICU admission, and 88 (30.6%) discharged home. Among the 68 initially at-risk patients who returned, 54 (79.4%) were admitted to general floor, 1 (1.5%) was admitted to the ICU, and 13 (19.1%) were discharged home.
Conclusion(s): Pediatric patients discharged home after an ED visit with positive sepsis risk screen had higher rates of infectious return visits and hospital admission within 30 days compared to those without sepsis risk. These findings suggest that an initial positive sepsis risk screen may identify children at increased risk for clinical deterioration after discharge, highlighting the importance of targeted follow-up and risk-based discharge strategies.
Table 1. Demographics and Clinical Characteristics
Table 2. Return visits within 30 days with ICD-10 diagnosis of infectious etiology
Table 3. ED Disposition of return visits with ICD-10 diagnosis of infectious etiology


.png)