Session: Neo-Perinatal Health Care Delivery: Epidemiology/Health Services Research 2
98 - The Association Between Maternal Birth Country and Race with Infant Mortality
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3094.98
Folasade Aderibigbe, University of Alabama Birmingham, Birmingham, AL, United States; Waldemar Carlo, University of Alabama, Birmingham, AL, United States; Colm P. Travers, University of Alabama at Birmingham, Birmingham, AL, United States
University of Alabama Birmingham Birmingham, Alabama, United States
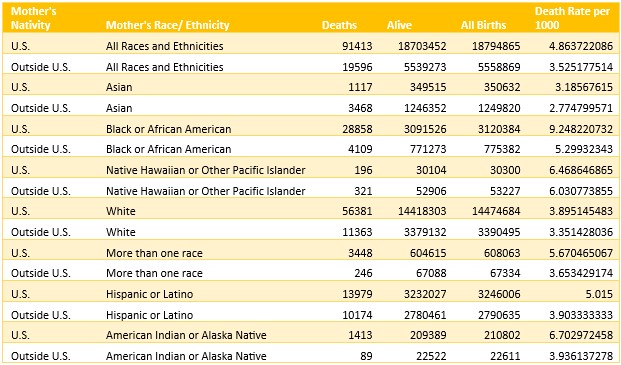
Background: There are well documented differences in adverse pregnancy outcomes among US born mothers compared to their non-US born counterparts. There is a paucity of data evaluating the association between maternal nativity and infant mortality rates (IMR) in the US by race and ethnicity. Objective: We hypothesized that Infants born to mothers who were born in the US would have higher IMR compared with infants of non-US born mothers by race and ethnicity. Design/Methods: This cohort study utilized population-based data from the Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER) expanded linked birth and infant death records database for 2017-2023. We included all hospital-born live births with gestational age 21 to 42 weeks from 2017-2023. Gestational age was defined using last menstrual period. The primary analysis compared the infant mortality rate per 1000 live births between US born and non-US born mothers by race and ethnicity. Chi-square was used to analyze the association between exposure (maternal nativity) and the IMR. A two-sided p value of less than 0.05 was considered significant. Results: We included 24,353,734 infants, of whom 18,794,865 (77.2%) were delivered to US-born mothers and 5,558,869 (22.8%) delivered to non-US born mothers. Overall, infants born to US-born mothers had a higher risk of IMR compared to infants born to non-US born mothers 4.86 versus 3.53; p< 0.0001). There was a significant difference in IMR for each race and ethnicity included favoring infants of non-US born mothers (all p< 0.0001). Infants of US-born Black mothers had the largest absolute difference in IMR compared with non-US born Black mothers (9.25 versus 5.30; p< 0.0001). Infants of US-born Asian mothers had the smallest absolute difference in IMR compared with their non-US born counterparts (3.19 versus 2.77; p< 0.0001).
Conclusion(s): This study using population-based data suggests that infants that are born to US-born mothers have higher IMR compared to infants of foreign-born mothers across all racial and ethnic groups. The disparity was largest among infants born to US-born Black women compared with infants born to non-US born Black women.