Session: Neonatal General 7: Cardiology and Hemodynamics
429 - Effect of Different Intervals to Umbilical Cord Clamping at Birth on
Arterial Cord Gases
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3414.429
Dhuha S Z A F. Alajmi, Dalhousie University Faculty of Medicine, Halifax, NS, Canada; Tim Disher, IWK Health Centre, West Porters Lake, NS, Canada; John Fahey, Children's Specialized Hospital, Halifax, NS, Canada; Balpreet Singh, Dalhousie University Faculty of Medicine, Halifax, NS, Canada; Melissa Brooks, Dalhousie University Faculty of Medicine, Hafifax, NS, Canada; Azar Mehrabadi, Dalhousie University, Halifax, NS, Canada; Walid El-Naggar, Dalhousie University, Halifax, NS, Canada
Professor of Pediatrics Dalhousie University Halifax, Nova Scotia, Canada
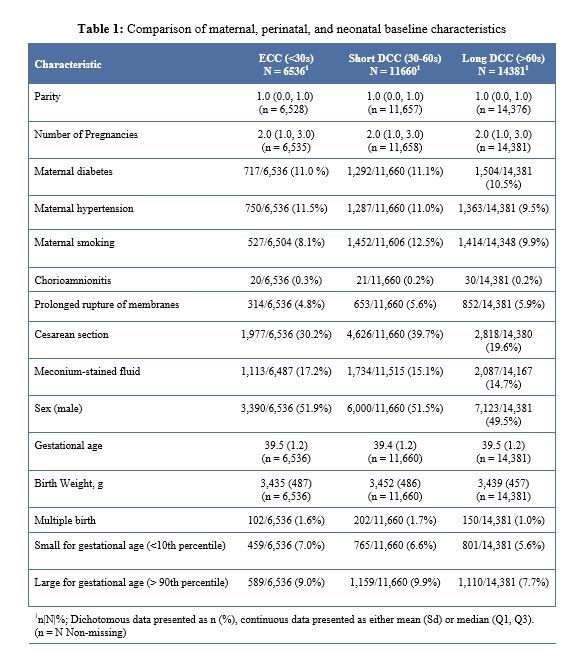
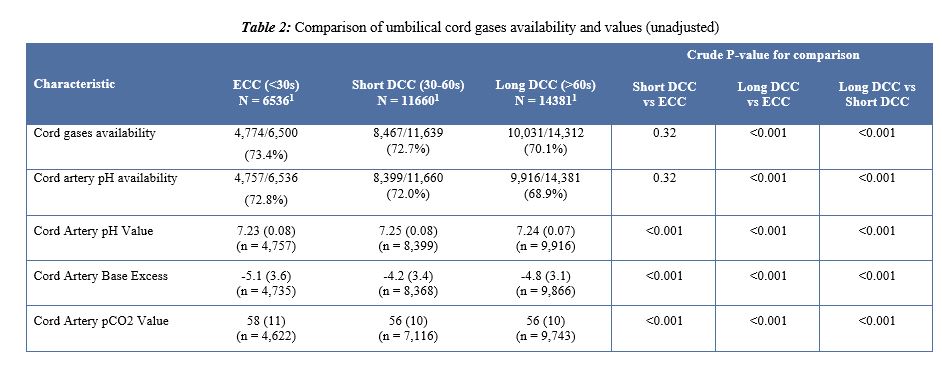
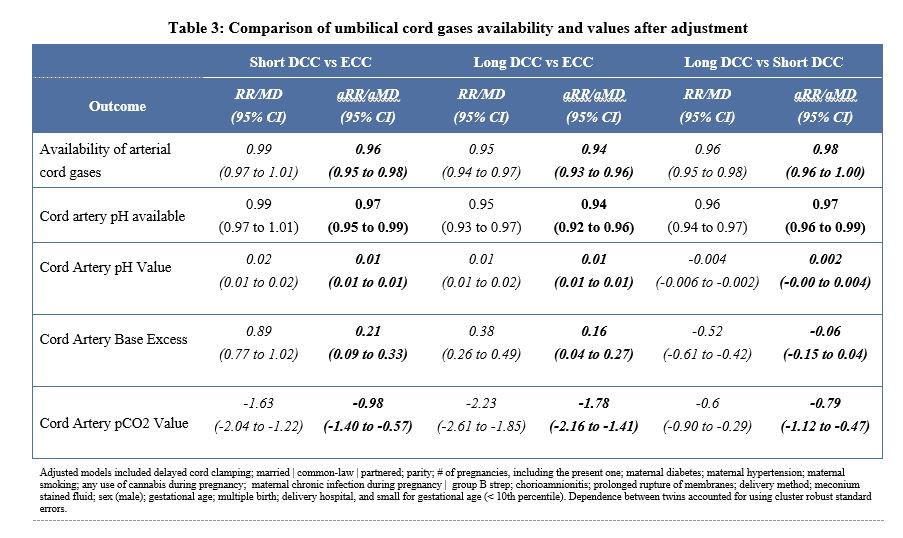
Background: Arterial cord gases are crucial for clinical and legal purposes. There is a controversy whether deferred cord clamping (DCC) at birth affects arterial umbilical cord gases availability and values in full-term infants. Objective: To investigate the impact of different intervals to cord clamping on the availability and values of arterial umbilical cord gases in full-term deliveries. Design/Methods: This population-based retrospective study included full-term infants born between 2018-2024 in the province of Nova Scotia, Canada. Obtaining umbilical cord gases is a standard practice in all deliveries. We excluded deliveries of infants with major congenital anomalies, fetal anemia, born after placental abruption and those who had umbilical cord milking. Study population was categorized into 3 groups based on the duration to cord clamping (early cord clamping, ECC < 30 sec, short DCC 30-60 sec, long DCC > 60 sec). Maternal & perinatal characteristics and availability and values of umbilical cord gases were compared. Logistic regression models were used to compare the outcomes among the three groups adjusting for prespecified confounders. Results: A total of 32,577 infants were included at a mean gestational age 39.5 weeks. Of these, 6,536 (29.1%) received ECC, 11,660 (35.8%) received short DCC and 14,381 (44.1%) received long DCC. Maternal and neonatal characteristics are shown in Table 1. Arterial cord gases were available in 73.4% of the ECC group, 72.7% of the short DCC group and 70.1% of the long DCC group (Table 2). After adjustment for potential confounders, short and long DCC were associated with increased risk of unavailability of umbilical cord gases compared to ECC [aRR (95% CI) 0.96 (0.95 to 0.98) and 0.94 (0.93 to 0.96)]-Table 3. There were statistically significant differences in arterial cord pH, pCO2 and base excess values between the 3 groups.
Conclusion(s): This large population-based study shows that the availability of arterial cord gases was reduced by increasing durations to cord clamping. However, this minor reduction should be weighed against the multiple benefits of DCC especially that those who receive longer DCC are usually stable healthy infants. The resulting differences in arterial cord gas values, though statistically significant, may not be of clinical significance.
Table 1 - Comparison of maternal, perinatal, and neonatal baseline characteristics
Table 2 - Comparison of umbilical cord gases availability and values (unadjusted).
Table 3 - Comparison of umbilical cord gases availability and values after adjustment.