52 - Substance Use Disorder Screening and Follow-Up in a Virtual Maternity Program Across Rural and Urban Residents
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3049.52
Ian J. Hooley, Pomelo Care, New York, NY, United States; Lena Bertozzi, Pomelo Care, New York, NY, United States; Isabelle von Kohorn, Pomelo Care, Washington, DC, United States; Stacey Kallem, Pomelo Care, Merion Station, PA, United States; Sara Handley, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Head of Pediatrics Pomelo Care Merion Station, Pennsylvania, United States
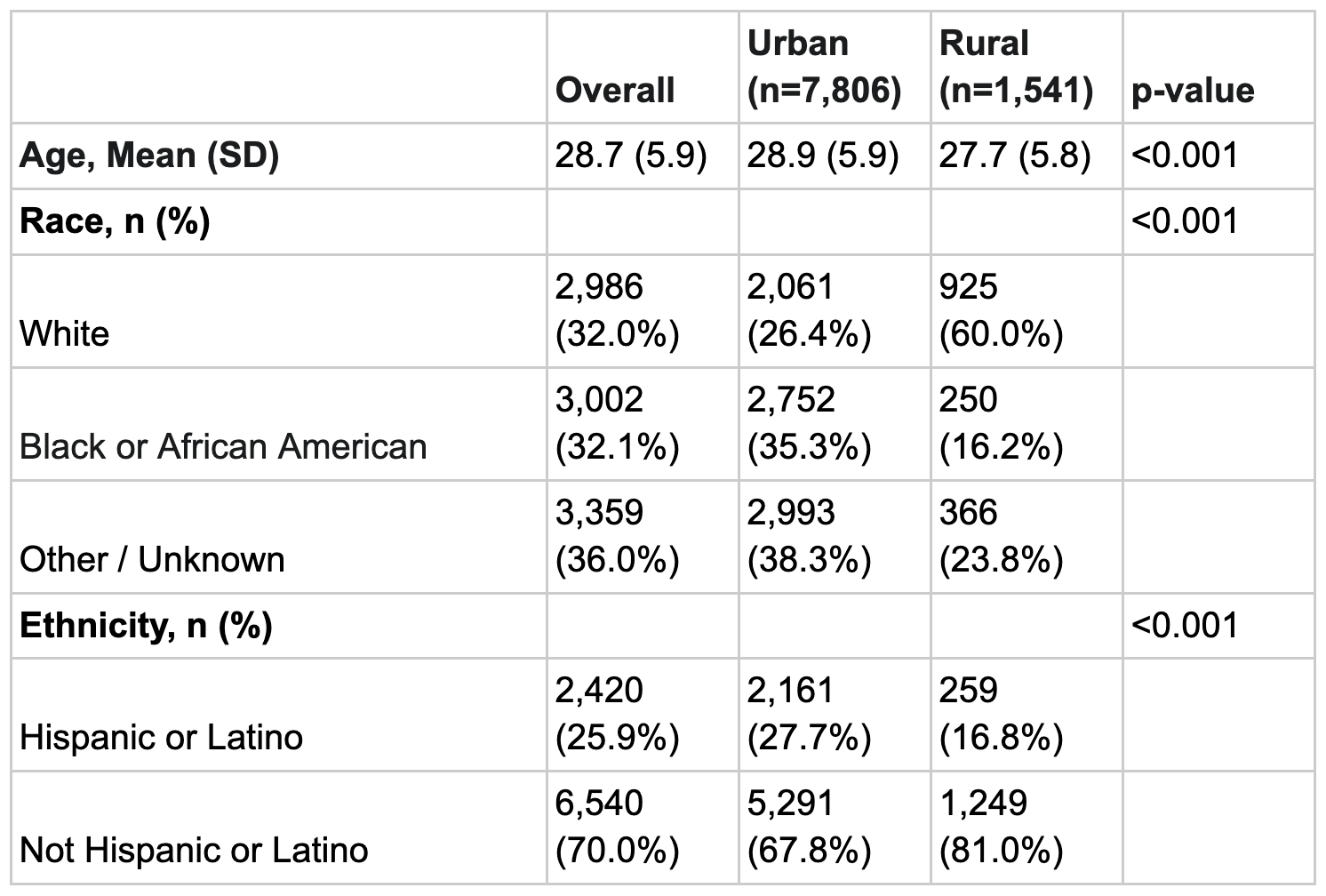
Background: Substance Use Disorder (SUD) is a leading, preventable cause of maternal and neonatal morbidity. While universal screening with a validated tool is recommended, implementation remains low. SUD rates are often higher among rural residents, who also have less access to care. Virtual care models may offer a scalable method to bridge these gaps by standardizing evidence-based screening and follow-up. Objective: To evaluate a virtual maternity program's impact on SUD screening, SUD prevalence, and follow-up rates, comparing outcomes between rural and urban residents in a Medicaid and commercially insured population. Design/Methods: This retrospective quality improvement analysis included 9,347 pregnant individuals from 36 states (Jan 2024-Jun 2025) who enrolled in a virtual maternity program. The cohort included patients with 1+ visits. Residence was categorized by USDA Urban Influence Codes (Rural vs. Urban). Demographic differences across the groups were analyzed. Virtual SUD screening was implemented using the TAPS (Tobacco, Alcohol, Prescription, and other Substance) tool. The primary outcomes were screening rate and substance-specific positive screen prevalence. Secondary outcomes were follow-up rates at 24 hours and 30 days post-positive screens, as measured through clinical engagement with the virtual maternity program (message, video or audio visit). Chi-square tests were used to assess significance. Results: Rural patients were significantly younger (27.7 vs 28.9 years, p< 0.001) and more likely to be White (60.0% vs 26.4%, p< 0.001) than urban patients (Table 1). The overall SUD screening rate was 82.3% (7,695/9,347). Screening rates were equitable across geographic groupings (Rural: 82.1% vs. Urban: 82.4%; p=0.82). Among those screened, rural patients had a significantly higher prevalence of any positive SUD screen (54.8% vs. 40.8%; p< 0.001), driven by higher prevalence of positive tobacco (41.2% vs. 24.5%; p< 0.001) and illicit drug (15.8% vs. 13.7%; p=0.048) screens. Among 3,318 patients with a positive screen, 84.8% received follow-up within 24 hours and 96.9% within 30 days (Table 2).
Conclusion(s): A virtual maternity program achieved high rates of validated screening and follow-up for SUD at both 24 hours and 30 days. Rates were equal in rural and urban patients, despite different baseline demographics and a higher prevalence of SUD (tobacco, illicit drugs) among rural patients. These results demonstrate that virtual maternity care is an effective solution to achieve high rates of evidence-based screening and follow-up for SUD to overcome geographic barriers to care.
Table 1: Cohort Sociodemographic Characteristics
Table 2: Program SUD Screening, Prevalence, and Follow-Up Rates by Population

 photo")
.png)
