144 - A Quality Improvement Initiative to Reduce Unplanned Extubations in the NICU
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3138.144
Hasene Ozlem. Kasaroglu, Women & Infants Hospital of Rhode island, Milton, MA, United States; Avery Zierk, Women & Infants Hospital of Rhode Island, Providence, RI, United States; Laurie Hoffman, Women & Infants Hospital of Rhode Island, Providence, RI, United States; Abbot R.. Laptook, Women & Infants Hospital of Rhode Island, North Kingstown, RI, United States; Nicholas G.. Guerina, Women & Infants Hospital of Rhode Island, Providence, RI, United States
Attending Neonatologist Women & Infants Hospital of Rhode island Milton, Massachusetts, United States
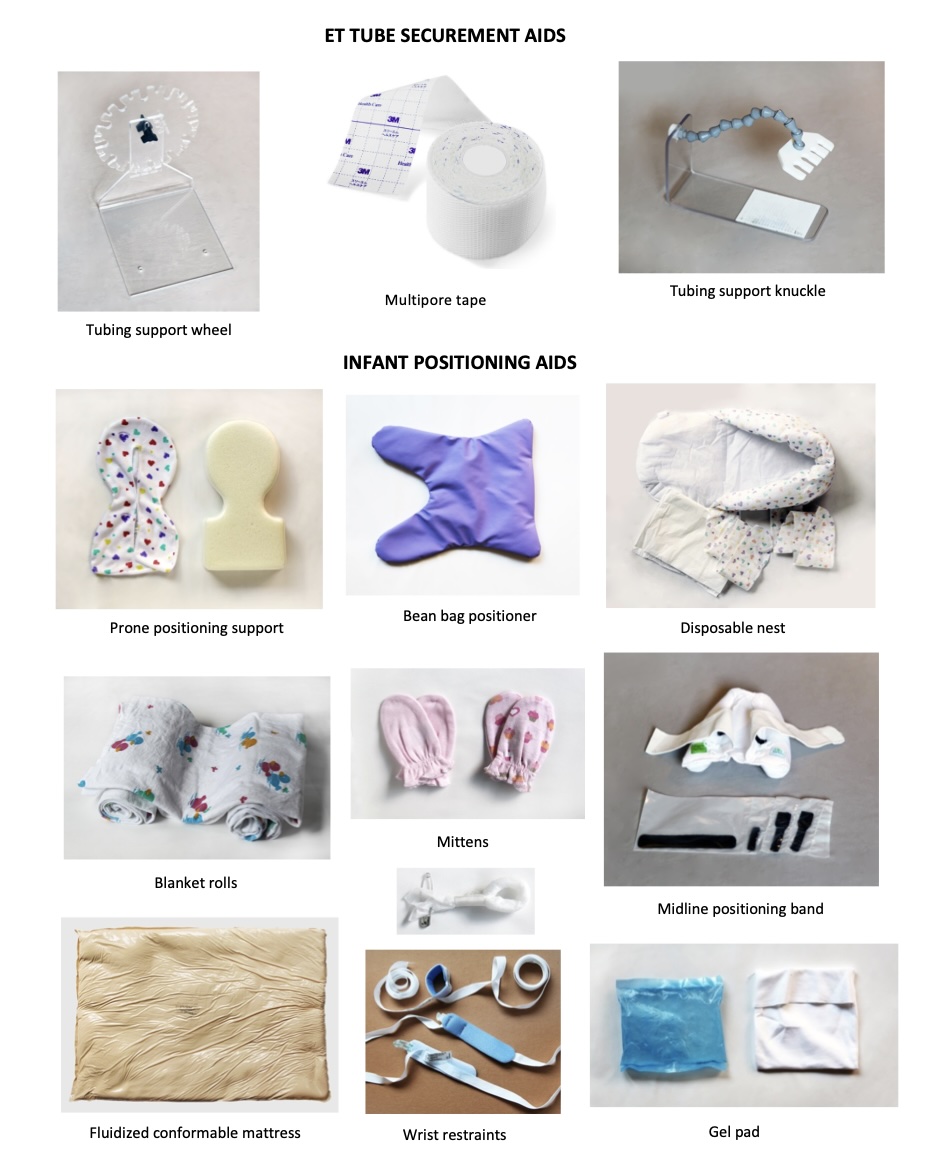
Background: Unplanned extubation (UE) is a frequent and potentially serious event associated with adverse outcomes. Objective: Our aim was to reduce UEs per 100 ventilator days from its current rate of 2.1 to 1.0 by 1 year through development and implementation of a standardized intervention package. Design/Methods: This quality improvement (QI) initiative was completed in an 82-bed level IV NICU. The primary outcome measure tracked was UE events per 100 ventilator days. Baseline data was collected from 1/14 through 10/15. An intervention package was developed between 10/15 and 8/16 that included standardized ETT securement and infant positioning aids, reinforcement of the two-person requirement for ETT care, ETT adjustment, infant movement and repositioning, and staff re-education via PowerPoint modules and video demonstrations (Figure 1). Implementation took place 9/16 through 5/17. Continued UE tracking (6/17-12/17) informed a second phase of training with bedside pictorial guides and electronic medical record (EMR) fields for documentation (1/18-3/18). Process measures included percent of package interventions present during UE events. Identified factors contributing to UE events were tracked during the baseline period as well as during the implementation and sustain phases of the project (Table 1). Results: Special cause variation in the outcome measure was seen starting in 8/19 with the average UE rate decreasing from 2.1 to 0.7 shown in an XmR statistical process control chart (Figure 2). This improvement has been sustained through 6/24. Documentation showed recommended ETT securement aids in use 87% and positioning aids at 59% of the time during UEs.
Conclusion(s): An intervention package emphasizing standardization, staff reeducation, and real time documentation led to a sustained reduction in UE events. Ongoing monitoring of UE events and process measures may further identify opportunities for procedural improvements.
Figure 1. ETT Securement and Infant Positioning Aids
Table 1. Percent of UE events per identified contributing factors.

 Credit")
 photo")
.jpg)

