297 - Pediatric Mental Health Utilization After Military Sponsor, Spouse, or Child Injury
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3286.297
Julianne LeGierse, Uniformed Services University of the Health Sciences F. Edward Hebert School of Medicine, Bethesda, MD, United States; Ian S. Sorensen, HJF, Bethesda, MD, United States; Kalyn C. Jannace, Uniformed Services University of the Health Sciences F. Edward Hebert School of Medicine, Bethesda, MD, United States; Elizabeth Hisle-Gorman, Uniformed Services University, Bethesda, MD, United States; Sarah Prabhakar, HJF, Bethesda, MD, United States; Rebecca Schulz, Uniformed Services University of the Health Sciences F. Edward Hebert School of Medicine, Rockville, MD, United States
PhD Student Uniformed Services University of the Health Sciences F. Edward Hebert School of Medicine Bethesda, Maryland, United States
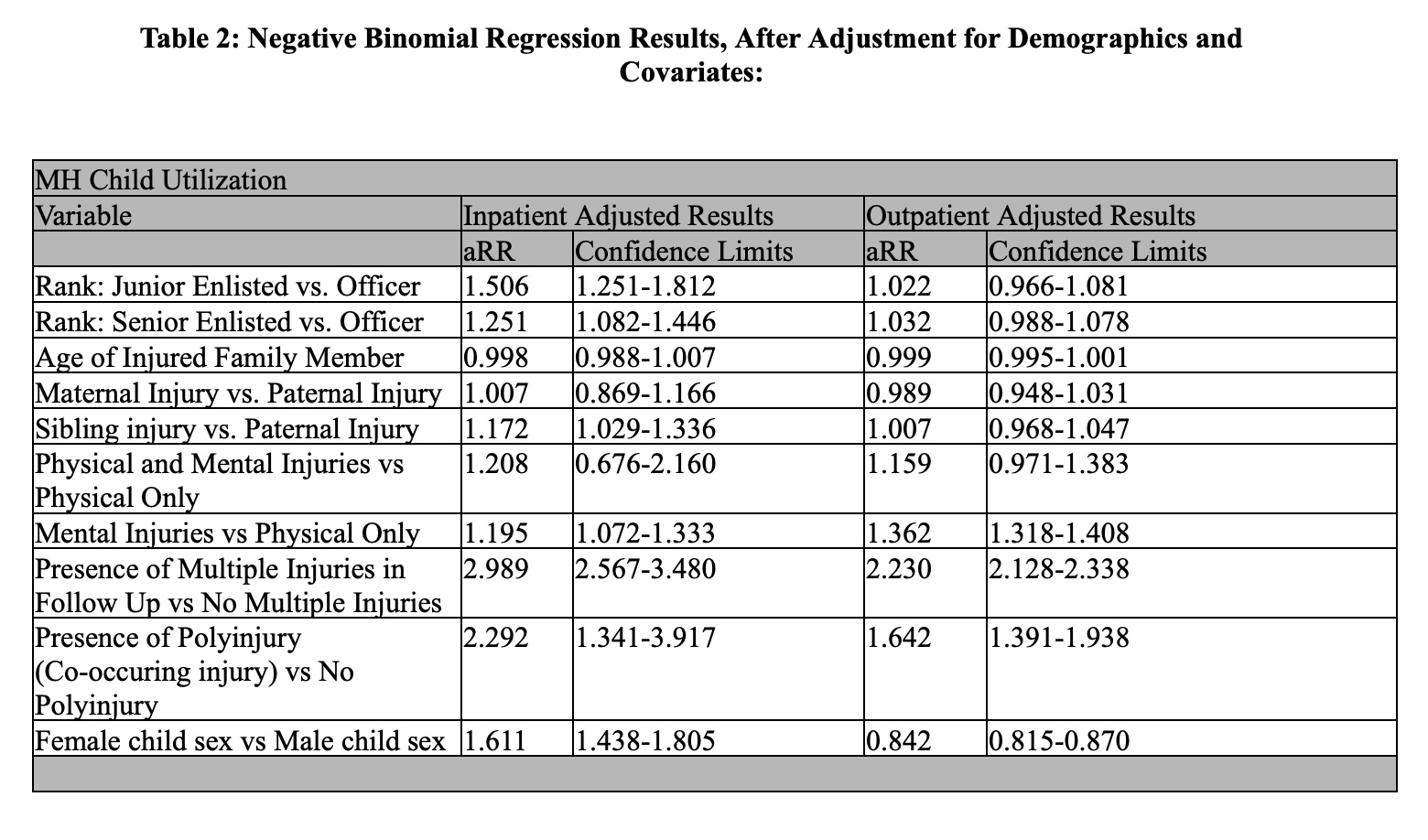
Background: Family member serious injury can add stress to family systems. Previous research has associated parental injury with increased mental health (MH) care by their children. Little is known about how family role, injury type, and severity impact MH care need. Objective: To determine the impact of family role, injury type and injury severity on the MH care needs of uninjured children in the family. Design/Methods: Electronic health record data, obtained through the Military Health System Data Repository, identified people who experienced a serious injury between 2005 and 2015 and their family members, including uninjured children. Pediatric inpatient and outpatient MH care were tallied for the 5 years after the family member's injury. The type of injury, family role (mother or sibling vs father), number of family members injured, and the presence of multiple family injuries (polyinjury) were quantified. Negative binomial regression models calculated rate ratios (RR) and 95% confidence intervals (CIs) for MH care among children aged 0-18. Adjusted models controlled for military member rank (an income surrogate), race, child age, and child sex. Results: 107,410 children were included. Physical (51%) injuries were most common followed by MH (48%), with 0.8% experiencing both injury types. Injuries were most common in fathers (40%), then siblings (35%) and mothers (25%), polyinjury impacted 1%, and 15% of families had more than one member injured (Table 1). Sponsor race was most often White (56%) and rank most often Senior enlisted (66%, middle income). Children were more likely to be female (52%); median age was 7. In adjusted models having an injured sibling (vs father) was associated with increased inpatient (aRR: 1.20, 95% CI: 1.07-1.33) but not outpatient care, and did not differ by maternal vs paternal injury. Inpatient and outpatient care was increased with family member MH injury by 20% and 36% respectively, with multiple family members injured (3.00 [2.57-3.48]; 2.23 [2.13-2.34 respectively), and with polyinjury (2.29 [1.34-3.92]; 1.64 [1.39-1.94) respectively). Inpatient care differed by race and rank, and outpatient care by race (Table 2).
Conclusion(s): Provider knowledge of mental health injury types, multiple individuals injured, and polytrauma as risk factors in families affected by injury may be important to identifying families at the highest risk and delivering appropriate mental health care to uninjured children.
Table 1: Mental Health Demographics by Injury Category, Rank, Role, Child Age and Sex
Table 2: Negative Binomial Regression Results, After Adjustment for Demographics and Covariates

.jpg)
.jpg)
