Clinical Research Fellow Cleveland Clinic Children’s Cleveland, Ohio, United States
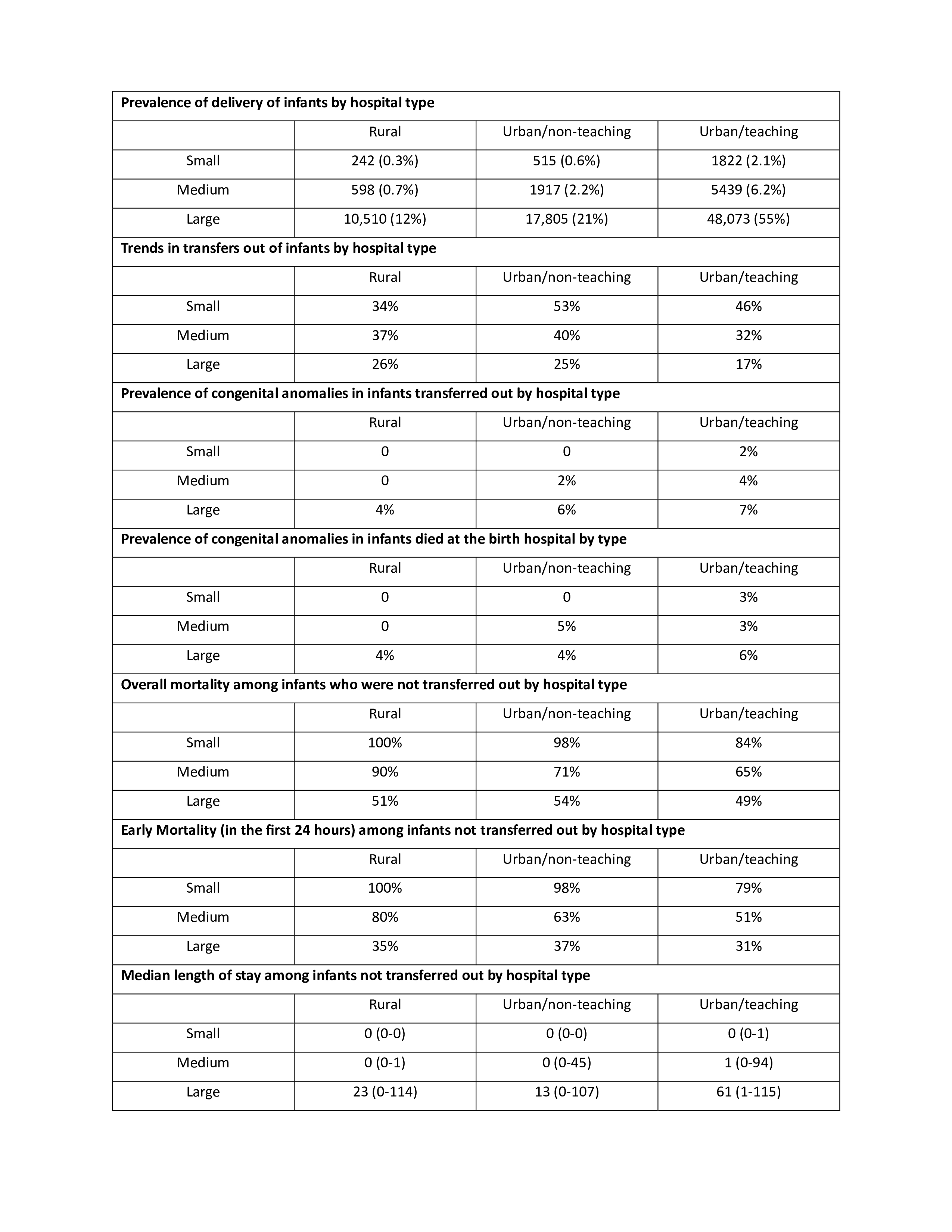
Background: There is inconsistency in reports describing the mortality among infants with gestational age (GA) < 26 weeks. Objective: To examine trends in hospital practices in resuscitating infants at the edge of viability based on hospital bed size, rural/urban location, and teaching versus non-teaching designation. Design/Methods: The datasets produced by the Healthcare Costs and Utilization Project (HCUP) were analyzed for the years 2016-2022. Infants < 26 weeks GA and < 1000g birthweight (BW) were included. Birth hospitals are categorized in the datasets based on rural vs. urban location and academic or teaching vs. non-teaching into 3 categories: rural, urban non-teaching, and urban teaching hospitals. Further, birth hospitals are classified according to bed-size into small, medium, or large hospitals. A matrix that combines both classification was created and was used to examine hospital practices. Results: Sample included 86,921 infants. Of them, infants < 23wk were 23.9%, 23wk were 19.6%, 24wk were 27.5%, and 25wk were 29%. Infants transferred out were 22.4%, those who expired at the birthing hospitals were 41%. Almost 2/3 of the deliveries occurred at urban teaching hospitals, while about 12% occur at large rural hospitals. Between 25-50% of the infants were transferred from the birth hospital. However, only 3-6% of infants transferred out have one or more severe congenital anomaly. The in-hospital mortality was 89.3%, 42.2%, 24.9%, and 15.6% in the < 23wk, 23wk, 24wk, and 25wk, respectively. More than 80% of infants were delivered at small or medium rural hospitals or small urban non-teaching or teaching hospitals who were not transferred out, expired. Similarly, the prevalence of congenital anomalies among them ranged from 3-6%. Most of them expired within the first 24 hours of life.
Conclusion(s): About 90% of infants at the edge of viability delivered at large hospitals. Between 30-50% of infants delivered at small to medium size hospitals were transferred out with no significant impact of the presence of congenital anomalies. Almost 90-100% of infants who were not transferred out in small to medium size rural hospitals and small urban non-teaching hospitals expired and mostly in the first 24 hours. It is not clear if the death is associated with failure of resuscitation attempts or a conscious decision made not to resuscitate. These findings highlight the importance of considering the hospital designation and size when calculating and comparing mortality in infants at the edge of viability.

 photo")