465 - Post-Discharge Outcomes for Neonatal Intensive Care Unit Graduates with Home Tube Feeding - A Retrospective Single Center Study
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4456.465
Eva Proels, Mercer University School of Medicine, Macon, GA, United States; Rachael Aldridge, Mercer University School of Medicine, Sharpsburg, GA, United States; Chloe Gray, Mercer University School of Medicine, Macon, GA, United States; Kylie Tobey, Mercer University School of Medicine, Macon, GA, United States; Joleen Dako, Mercer University School of Medicine, Fayetteville, GA, United States
Medical Student Mercer University School of Medicine Macon, Georgia, United States
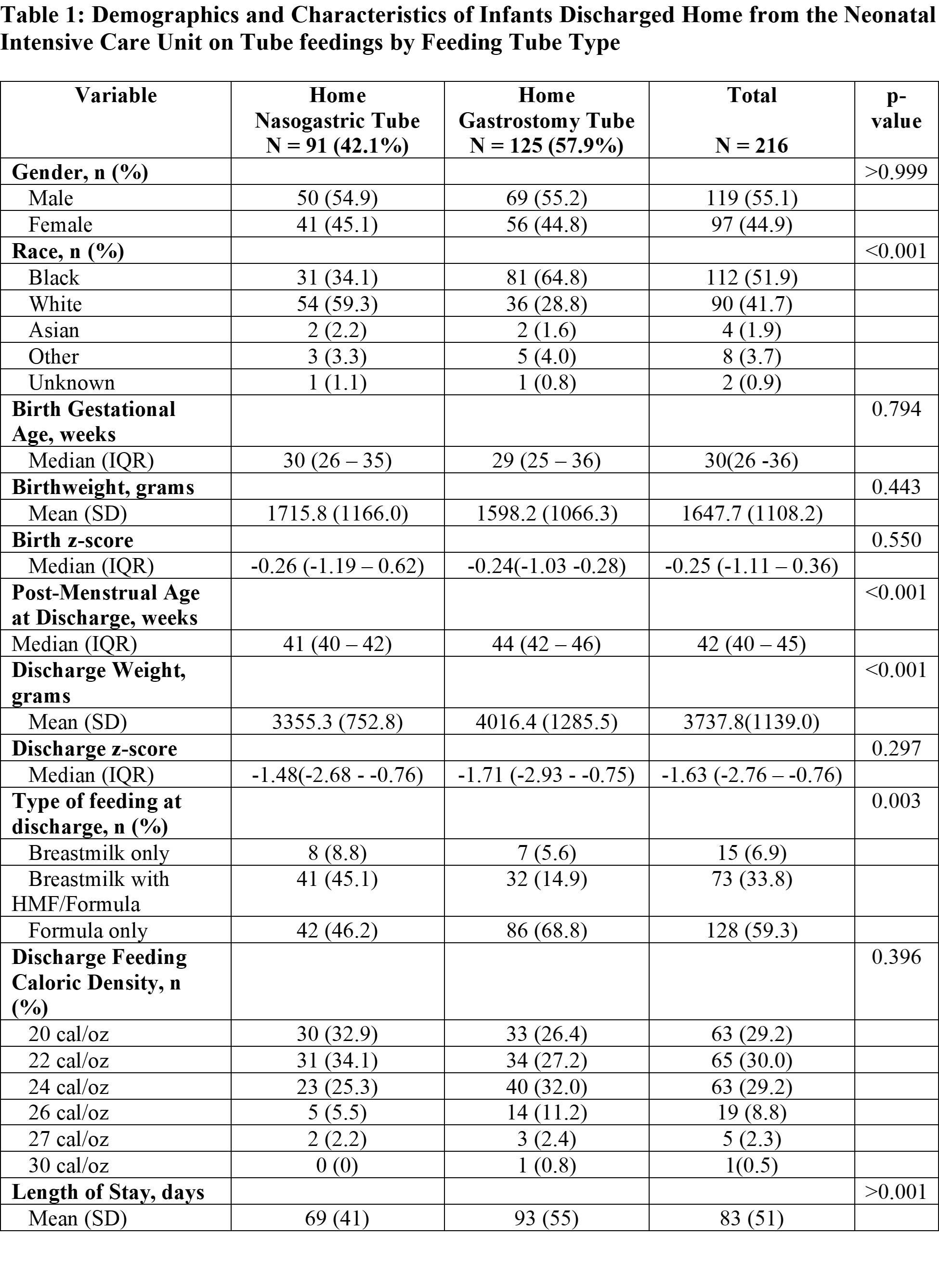
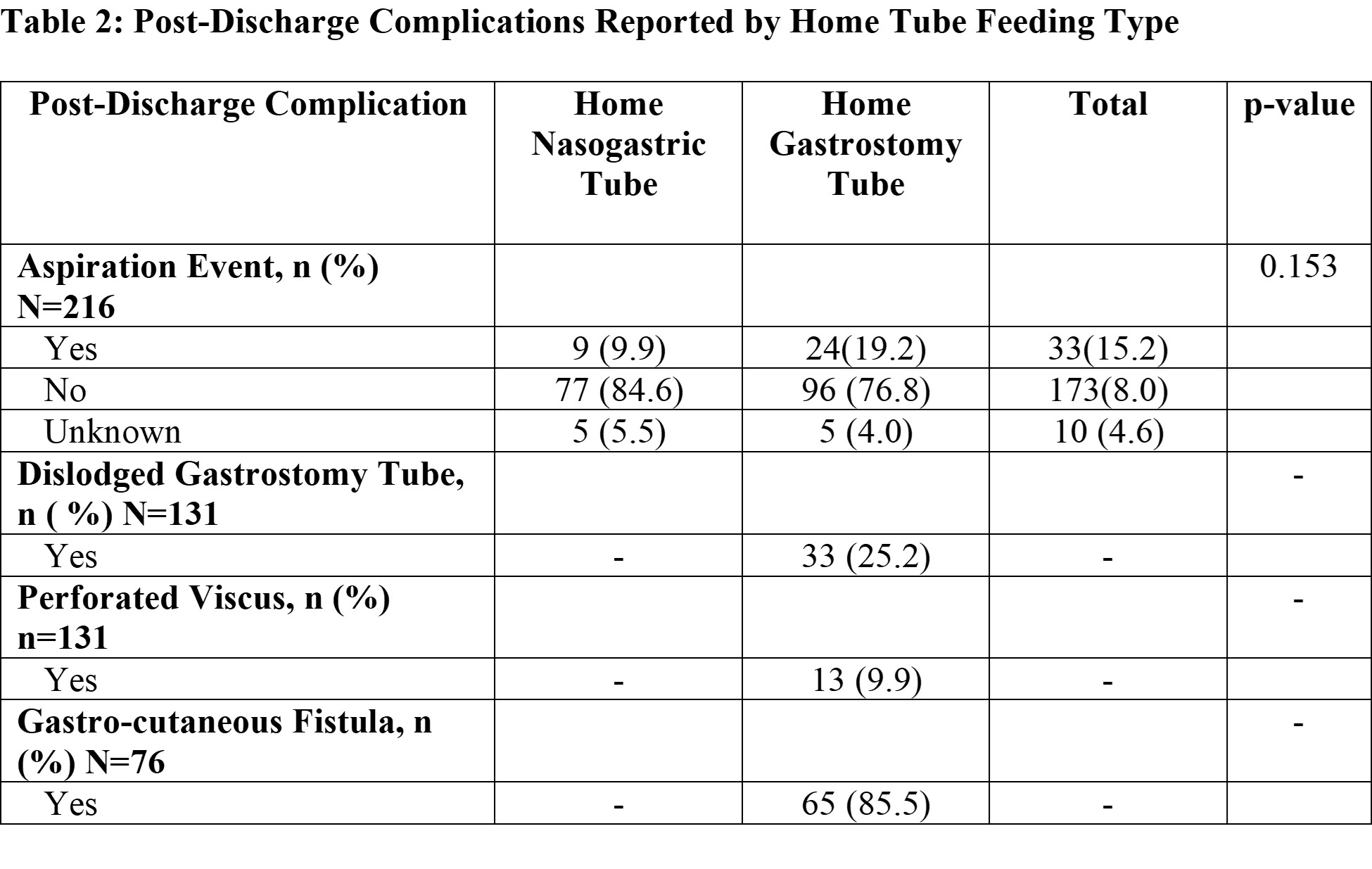
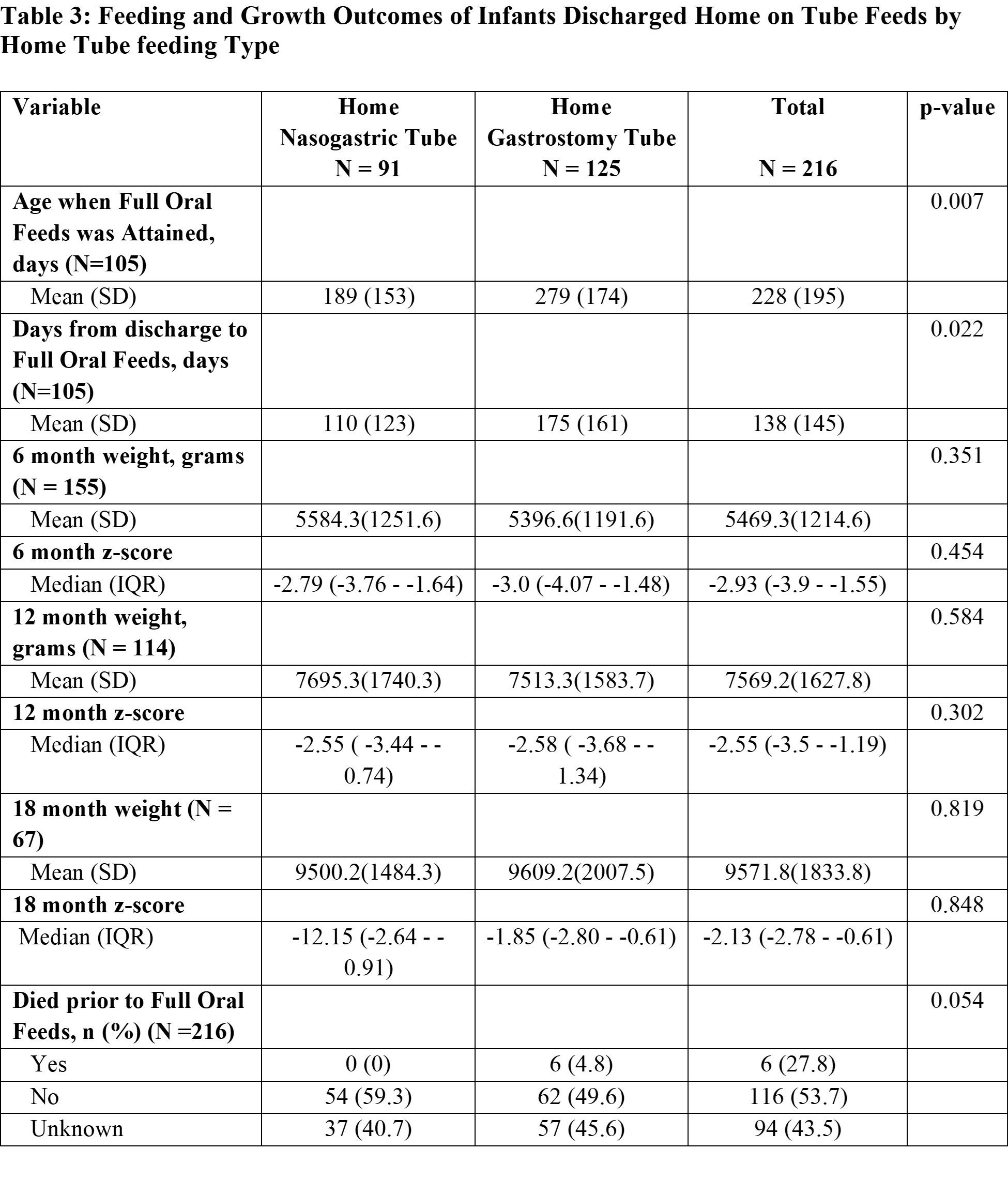
Background: Feeding problems can prolong Neonatal Intensive Care Unit (NICU) stay. Gastrostomy tubes (GT), which are surgically placed through the abdomen and nasogastric tubes (NGT), which are inserted through the nose are sometimes required for babies with dysphagia after discharge. Few studies have described complications and growth outcomes up to 12 months for infants discharged home on tube feeds. There is limited guidance on when to transition a patient from a NGT to a more long-term solution such as a GT. More studies are needed to describe the safety and efficacy of home tube feeding. Objective: To describe the duration of use of home feeding tubes by tube type and what proportion of babies require transition to GT after discharge home with NGT. We also describe growth outcomes and complications up to 18 months. Design/Methods: This was a retrospective chart review of neonates admitted to a level III NICU from July 1st, 2021, to July 31st, 2024, who were discharged home with tube feeds. We excluded infants transferred to the NICU primarily for GT placement. Infants' demographics, weights at 6, 12 and 18 months and complications reported at follow-up provider visits/calls were evaluated. Bivariate analysis of data was completed using Fisher's exact test and independent t-test. Results: 42% of the 216 infants included in the study were discharged home with NGT. Of these, 9% needed a GT after discharge. Babies discharged home with NG had shorter lengths of stay (p < 0.001) and required shorter duration of tube feeds post-discharge (110±123 vs 175±161 days, p = 0.02). Infants discharged home on tube feedings weighed approximately 2 standard deviations below average at 18 months. There were 6.5% with documented aspiration events. 25% of patients with GT reported dislodgement, 75% had a gastro-cutaneous (GC) fistula after removal of the GT and 64.5% required surgical closure of the GC fistula. Infants discharged home with NG differed by race and were more likely to be discharged home on some breast milk when compared to infants discharged home with a GT. 25% of infants included in the study were lost to follow-up, representing 34% of the NGT group and 18% of the GT group.
Conclusion(s): Majority of infants discharged home with NGT were adequately supported and never required a GT, while infants discharged home with GT often required a second surgery to repair a GC fistula after the GT was removed. There were no significant differences in growth outcomes at 6, 12 and 18 months for the 2 groups. This study may provide insight regarding home feeding strategies to providers and families in the NICU.
Table 1: Demographics and Characteristics of Infants Discharged Home from the Neonatal Intensive Care Unit on Tube feedings by Feeding Tube Type
Table 2: Post-Discharge Complications Reported by Home Tube Feeding Type
Table 3: Feeding and Growth Outcomes of Infants Discharged Home on Tube Feeds by Home Tube feeding Type