424 - Accuracy of Language for Care in the Pediatric ED
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4415.424
Elyse N. Portillo, Baylor College of Medicine, Houston, TX, United States; Colleen K. Gutman, University of Florida College of Medicine, Gainesville, FL, United States; Trishell Simon, Columbia University Medical Center/ New York Presbyterian, New York, NY, United States; Duc T. Nguyen, Baylor College of Medicine, Houston, TX, United States; Emily A. Hartford, University of Washington School of Medicine, Seattle, WA, United States; Peter Dayan, Columbia University, Hastings on Hudson, NY, United States; Victor M. de la Cruz, NewYork-Presbyterian Morgan Stanley Children's Hospital, Brooklyn, NY, United States; Tram N. Cao, Baylor College of Medicine, Houston, TX, United States; Marcela P.. Mendenhall, University of Colorado School of Medicine, Aurora, CO, United States; Alec S. Edid, University of Colorado School of Medicine, Denver, CO, United States; Kenneth Nobleza, Baylor College of Medicine, Houston, TX, United States
Assistant Professor of Pediatrics in Emergency Medicine Baylor College of Medicine Houston, Texas, United States
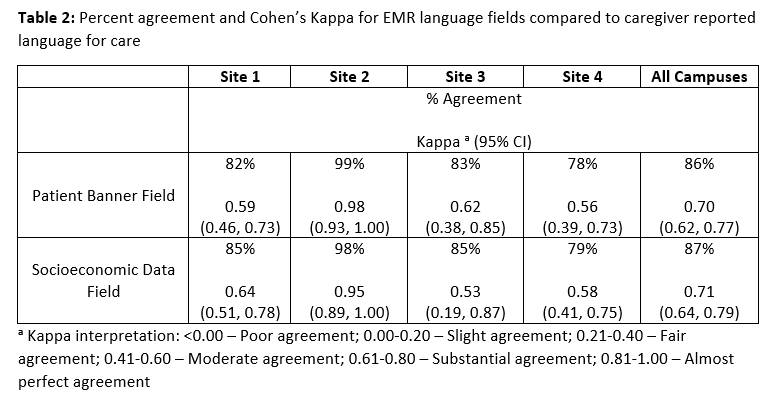
Background: Interpreter-mediated communication is crucial to provide high-quality care for patients who use languages other than English (LOE) for medical care. Timely engagement of interpreter services requires identification of language for care (LFC). Accurate and timely identification of a patient's LFC can be challenging, particularly during unscheduled, acute pediatric emergency department (PED) visits. Objective: As the first stage of a multicenter initiative to improve timely and accurate documentation of family LFC across four large, academic PEDs, we aimed to determine the missingness and accuracy of LFC documented in the electronic medical record (EMR) at the start of patient care. Design/Methods: We conducted a prospective 4-center study in two nodes of the Pediatric Emergency Care Applied Research Network, enrolling a convenience sample of ED patients from Oct 2024-2025. Exclusion criteria included patient age >19 years old, mental/behavioral health or abuse concerns, active resuscitation, or absence of legal caregiver. LFC was collected from two fields in the EMR, the patient banner and the socio-economic data language fields, at the start of clinical care, defined as provider assigned in the EHR for five minutes or less. Subsequently, caregivers were approached during the visit and reported preferred LFC. The agreement between each EMR-documented LFC field and caregiver report, as a measure for accuracy, was assessed by Cohen's kappa with 95% confidence intervals. Results: We screened two EMR fields, the patient banner field (n=464 patients) and the socio-economic data field (n=406 patients). Missing LFC at the start of clinical care ranged from 1-17% (Table 1). We approached 341 caregivers across the four sites to assess accuracy, of whom 103 (30%) reported LOE for medical care. Percent agreement of caregiver-reported LFC at the start of clinical care with EMR-documented fields ranged from 78% to 99% across sites (Table 2). Kappa statistics varied across sites, ranging from 0.53-0.98 (Table 2).
Conclusion(s): Missingness and accuracy of LFC documentation at the start of clinical care varied across PEDs. Findings will inform improvement interventions across sites, to ensure clinicians have the accurate LFC available when initiating patient care.
Table 1: Missingness in EMR language fields at the start of clinical care in ED encounters
Table 2: Percent agreement and Cohen's Kappa for EMR language fields compared to caregiver reported language for care

 photo")
.png)