408 - Use of emergency medical services for children with medical complexity
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4399.408
Sriram Ramgopal, Ann & Robert H. Lurie Children's Hospital of Chicago, CHICAGO, IL, United States; Carolyn Foster, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; MIchelle Macy, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Christopher Horvat, Carnegie Mellon University, Pittsburgh, PA, United States; Rebecca Cash, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States; Julia A.. Heneghan, University of Minnesota Medical School, Minneapolis, MN, United States; Allan M. Joseph, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Christian Martin-Gill, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States
Assistant Professor Ann & Robert H. Lurie Children's Hospital of Chicago CHICAGO, Illinois, United States
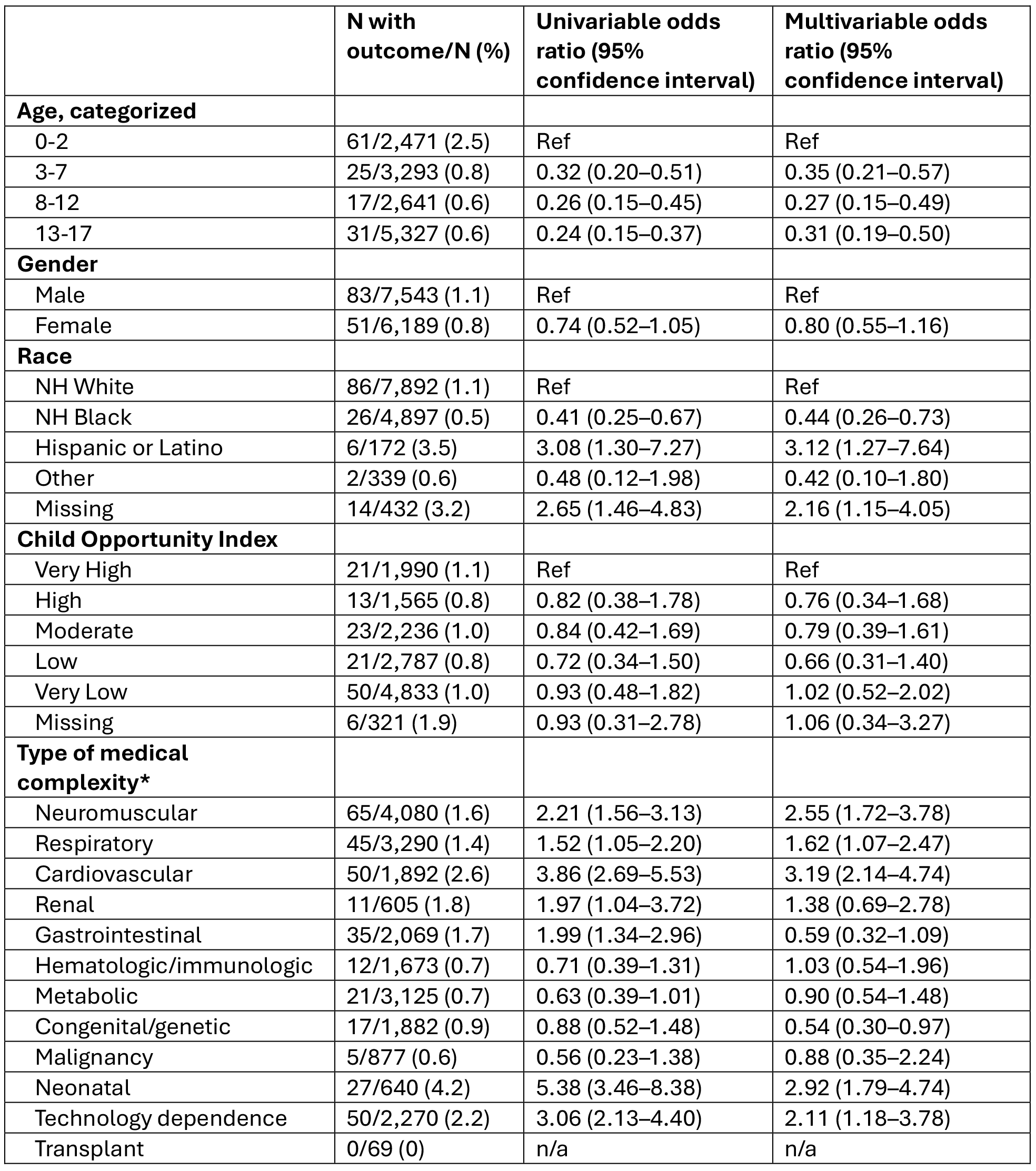
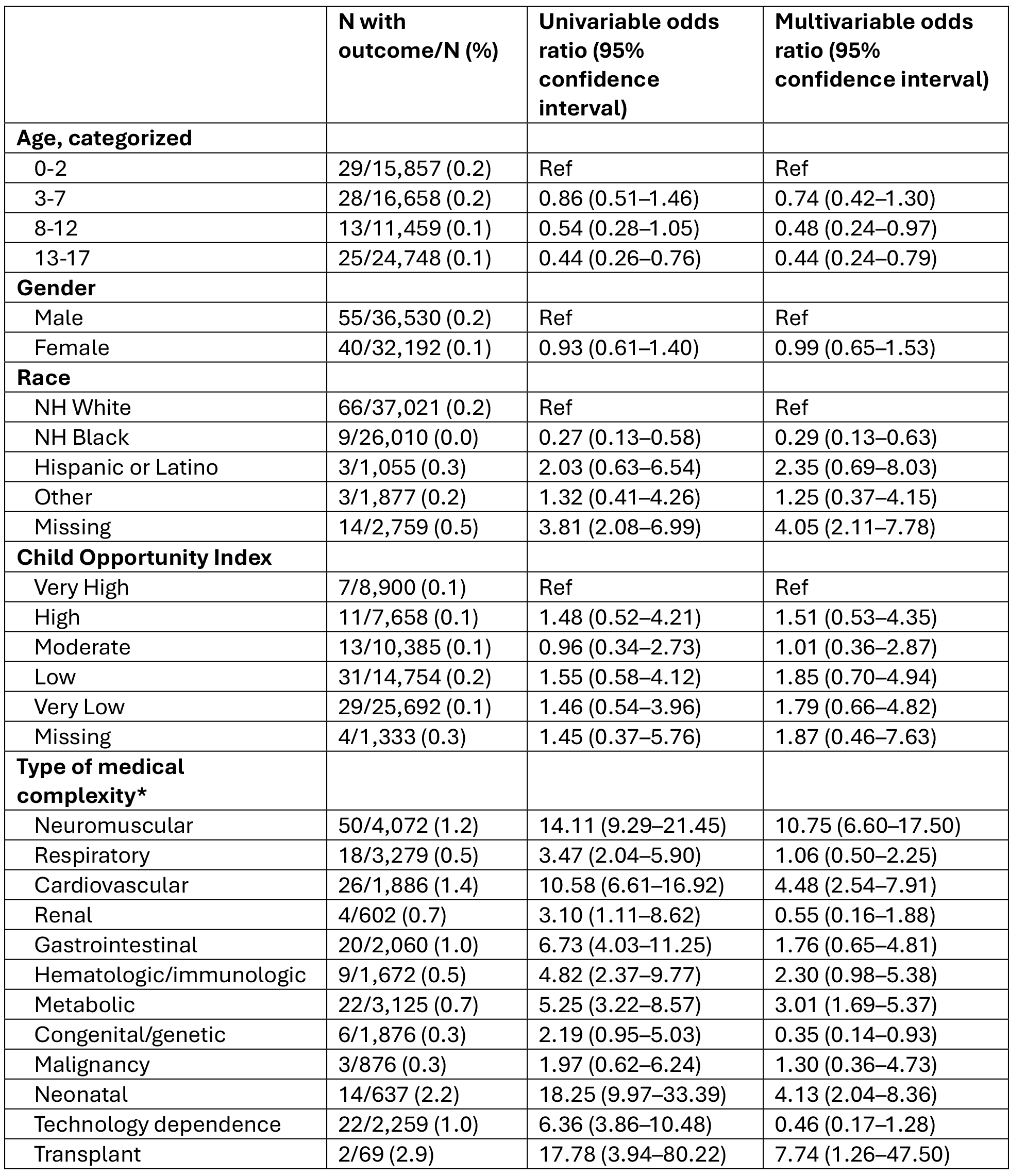
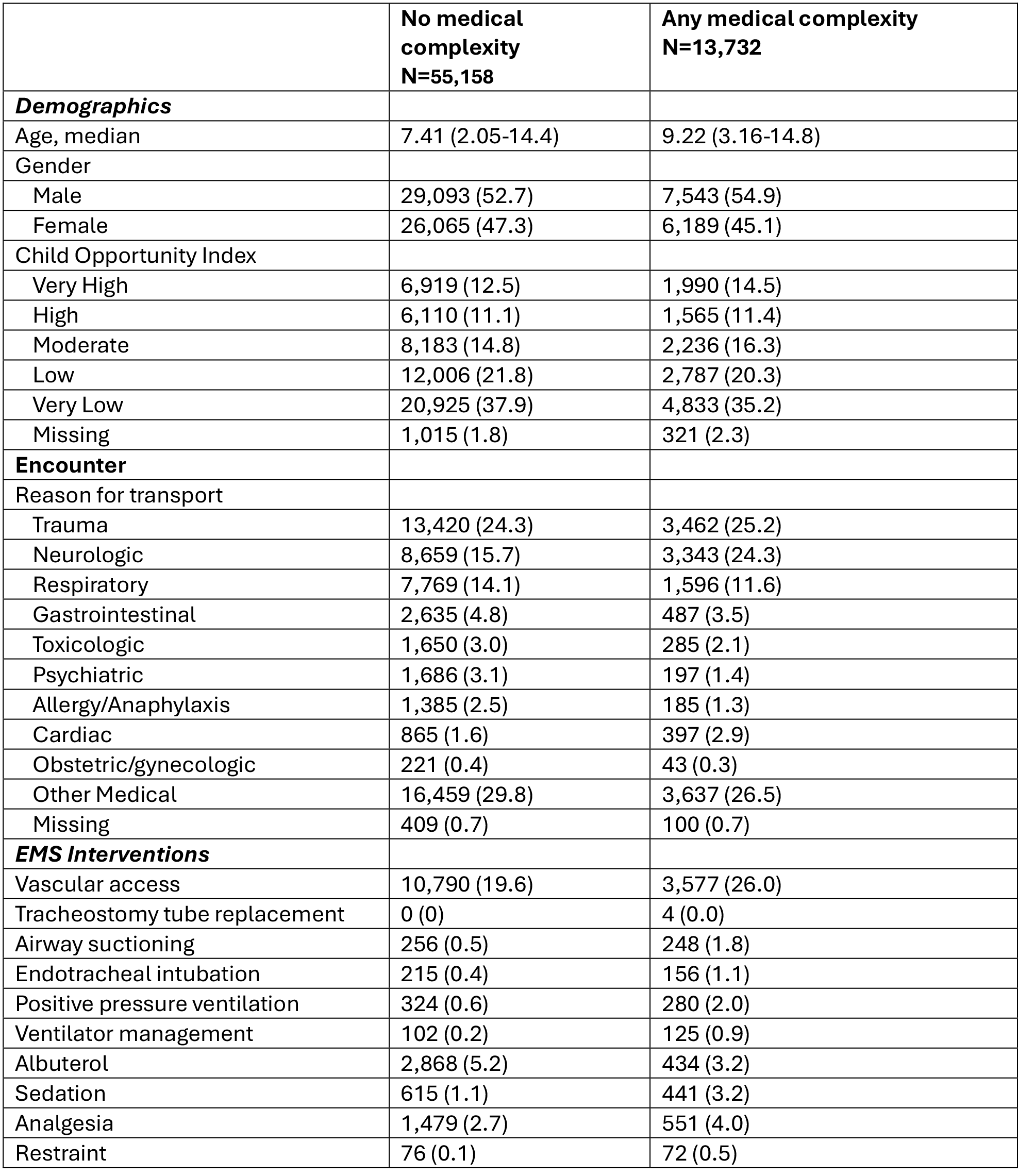
Background: For some medically complex children experiencing a health emergency in the community, emergency medical services (EMS) serve as the first point of contact with the healthcare system. Objective: To describe EMS utilization and care among CMC and to evaluate (a) factors associated with prehospital cardiac arrest CMC, and (b) the association of medical complexity with in-hospital mortality among children brought to the hospital by EMS. Design/Methods: We performed a multiagency study of children transported from the scene to one of 17 emergency departments (EDs) between 2014-2022, including community and academic settings and one pediatric hospital, within a regional EMS system. We used the Complex Chronic Conditions algorithm to identify CMC from ED and hospital diagnosis codes. We used generalized linear mixed models to evaluate factors associated with prehospital cardiac arrest among CMC and to assess the association of medical complexity with in-hospital mortality among children brought to the hospital by EMS. Results: Overall, 68,890 encounters were included (median age 7.8 years [IQR 2.2-14.5]; 53.2% males). At least one CCC type was present in 13,732 encounters (19.9%). The most common CCCs were for neuromuscular (4,080, 29.7%) and respiratory (n=3,290, 24.0%) conditions (Table 1). Among CMC, 134 (1.0%), had prehospital cardiac arrest. CCCs associated with greater prehospital arrest included cardiovascular (OR 3.19, 95% CI 2.14-4.74), neuromuscular (OR 2.55, 95% CI 1.72-3.78), and neonatal conditions (OR 2.92, 95% CI 1.79-4.74; Table 2). After removing all children with prehospital cardiac arrest who died in the ED (n=168), 95 (0.1%) had in-hospital mortality. The overall presence of medical complexity was associated with a 9.43 higher odds of in-hospital mortality (95% CI 5.96-14.91). Evaluating CCC types, neuromuscular (OR 10.75, 95% CI 6.60-17.50), cardiovascular (OR 4.48, 95% CI 2.54-7.91), and neonatal (4.13, 95% CI 2.04-8.36) conditions were associated with increased odds of in-hospital mortality (Table 3).
Conclusion(s): CMC comprise approximately 1 in 5 sampled EMS encounters. Risk of mortality varied by type of medical complexity, with the highest risk observed among children with neuromuscular conditions. These findings highlight the critical need for targeted EMS training and protocols that equip clinicians to recognize, stabilize, and manage the unique needs of CMC in the prehospital setting.
Table 1. Characteristics of encounters with and without medical complexity. Numbers represent median [IQR] or N (%).
Table 2. Association of medical complexity with in-hospital mortality in unadjusted and adjusted models.
Table 3. Factors associated with in-hospital mortality.

 photo")
 Numbers represent median [IQR] or N (%).
Numbers represent median [IQR] or N (%).