538 - Pegcetacoplan use in Pediatric Immune Complex-Membranoproliferative Glomerulonephritis (IC-MPGN), Dense Deposit Disease (DDD), Complement 3 Glomerulopathy (C3G): a Single Center Case Series
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4526.538
Emilia Maria Cadiz, Phoenix Children's Hospital, Phoenix, AZ, United States; Anjali Nayak, Phoenix Children’s Hospital, Phoenix, AZ, United States; Joshua Zaritsky, Phoenix children's hospital, Phoenix, AZ, United States; Katherine W. Perry, University of Arizona, Phoenix, AZ, United States
Pediatric Nephrologist Phoenix childrens hospial Phoenix, Arizona, United States
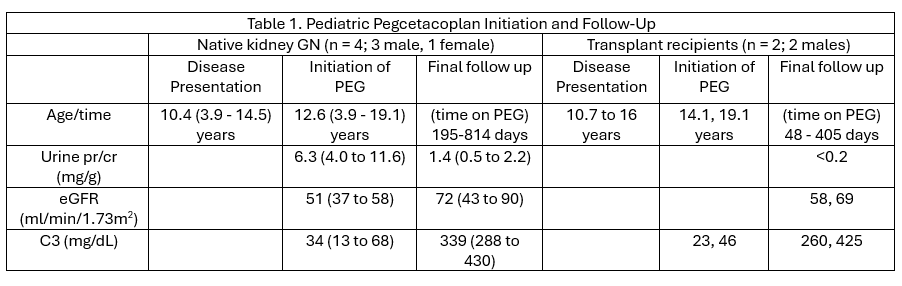
Background: C3G and primary IC-MPGN result from alternative complement pathway dysregulation. Persistent complement activation results in glomerular inflammation, progressive kidney damage, and end stage kidney disease (ESKD). C3G and IC-MPGN recur after kidney transplantation, leading to renal loss in most recipients. Pegcetacoplan (PEG), a C3 and C3b inhibitor, is approved for use in adults with C3G. It's use in children has been limited. Objective: To report our single center clinical experience with pegcetacoplan use in pediatric patients with C3G and IC-MPGN. Design/Methods: Demographic data, eGFR, urine protein excretion, and C3 levels were evaluated over time in 6 pediatric patients with C3G or IC-MPGN who received compassionate use or expanded access use of PEG. We used PEG in 4 patients (M=3; F=1) to treat active nephritis in their native kidneys. For 2 patients (M) with ESKD, we initiated PEG at the time of renal transplant to prevent disease recurrence. Patients were followed from 48 to 814 days after initiation of PEG. Results: In our patients with native kidney C3G, the average age was 10.4 years. On initiation of PEG, the average urine pr/cr was 6.3 mg/g, eGFR was 51mL/min/1.73m2, and C3 was 34 mg/dL. In our 2 transplant patients, we initiated PEG at age 14 and 19 years. C3 levels were 23 and 46, but increased to 260 to 425 on follow up. The two patients have not had any recurrence and urine pr/cr has been < 0.2mg/g. Other results can be seen in Table 1.
Conclusion(s): PEG controlled nephritis effectively in 6 pediatric patients with C3G/IC-MPGN. C3 levels increased 1277+353% in patients overall. In patients with active nephritis in their native kidneys, eGFR increased by 40+11% and proteinuria decreased by 73+6% with use of PEG. In renal allograft recipients treated with PEG, no disease recurrence was observed up to 405 days post transplantation.

 photo")