439 - Escaping a Stressful Reality: Parental, Patient and Child Life Specialist Perspective on Use of Virtual Reality in the Pediatric Emergency Department
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4430.439
Emily Berner, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Daniel Corwin, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Jane Lavelle, Childrens Hospital of Philadelphia, philadelphia, PA, United States; Frances Wood, Children’s Hospital of Philadelphia, Conshohocken, PA, United States; Erika L. Skesavage, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Olivia Fedio, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Jessica J. Albert, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Julia Fuchs, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Kristen C.. Lau, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Kristina Metzger, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Melissa R. Demock, Drexel University College of Medicine, Wyomissing, PA, United States; Laura Sartori, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Fellow Physician Childrens Hospital of Philadelphia Philadelphia, Pennsylvania, United States
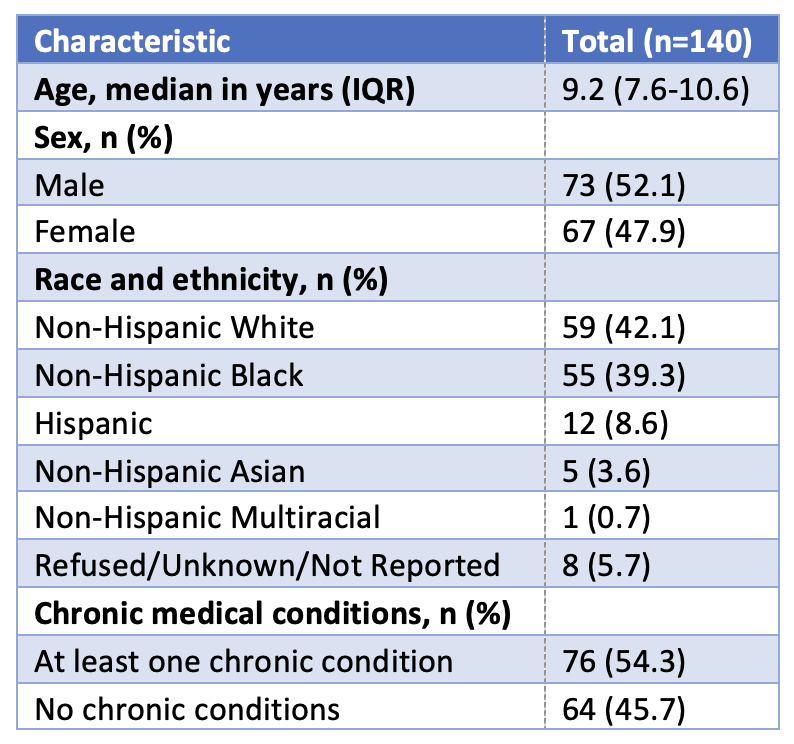
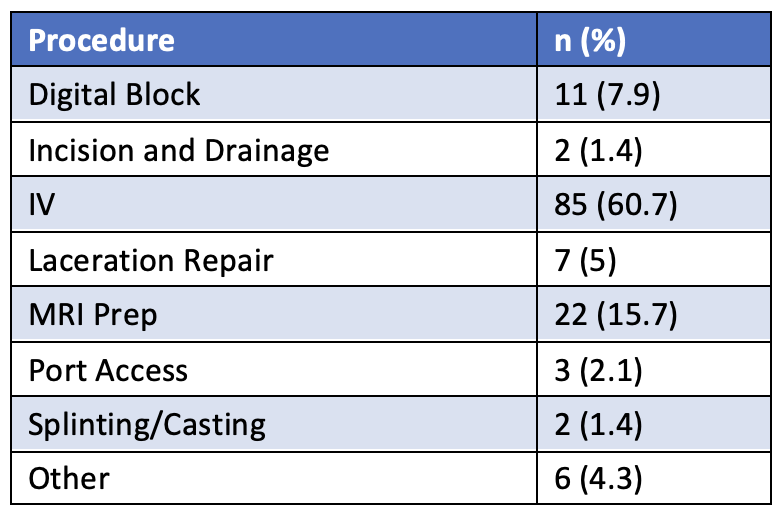
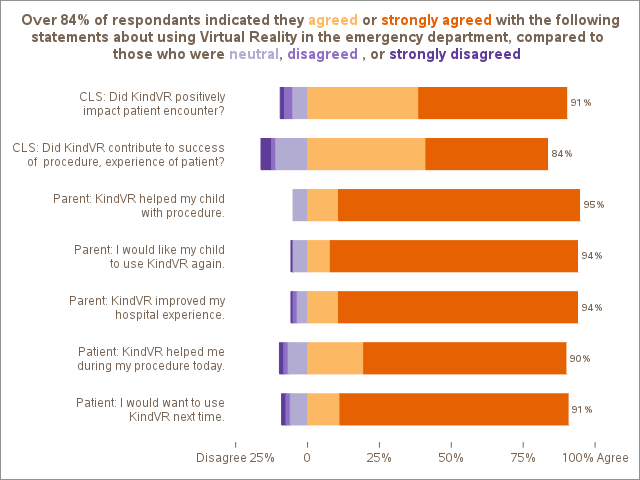
Background: The Emergency Department (ED) involves unplanned physically and emotionally taxing procedures, which can be stressful for patients and families. Virtual reality (VR) is an innovative, non-invasive immersive distractor technique shown to reduce procedure-related pain and anxiety. Child life specialists (CLS) guide patients through these stressful experiences, but their perspectives on VR use, and how this perspective aligns with the family experience, is poorly understood. Objective: Assess patient, parent, and CLS satisfaction following use of VR during painful or anxiety-provoking procedures in the pediatric ED. Design/Methods: Survey-based study of patients, parents and CLS following use of VR in the ED among typically-developing children aged 5 to 18 years at a large, tertiary care children's hospital from December 2024 to September 2025. Patients with high-acuity illness, significant atypical development limiting ability to engage with VR, aggressive behavior with potential to cause harm to self or others, and those with injury or infection to the head or eyes impacting ability to wear the device were excluded. Enrollment was limited to patients and families able to complete surveys in English. Eligible patients were identified by CLS in conjunction with the ED clinical team and CLS facilitated use of VR. Patients, parents, and CLS filled out Likert-scale questions immediately following the procedure. Results: We enrolled 140 triads of patients, parents, and CLS. Median age was 9.2 years (IQR 7.6-10.6 years) (Table 1) and the most commonly used procedure was IV insertion (n=85, 60.7%) (Table 2). Patients, parents, and CLS overwhelmingly agreed that VR was a helpful adjunct with 91% of CLS agreeing that VR positively impacted the patient encounter and >90% of parents and children agreeing that VR was helpful (Figure 1). 54.3% of patients had at least one chronic medical condition and success of procedure did not vary significantly based on presence of a chronic medical condition (p= 0.33). 8.6% of patients received anxiolysis and success of procedure did not vary significantly based on receipt of anxiolysis (p= 0.54).
Conclusion(s): Our results suggest that when used in conjunction with highly trained CLS, VR is an effective tool for improving the ED experience related to acute ED interventions. Future research should aim to explore the utility of VR for patients throughout the ED encounter, including in those with chronic pain for whom an immersive experience may be particularly beneficial.