
Neonatal Hemodynamics and Cardiovascular Medicine
Session: Neonatal Hemodynamics and Cardiovascular Medicine 5

Alyssa R. Thomas, MD
Attending Neonatologist
Brigham and Women's Hospital
SOUTH BOSTON, Massachusetts, United States
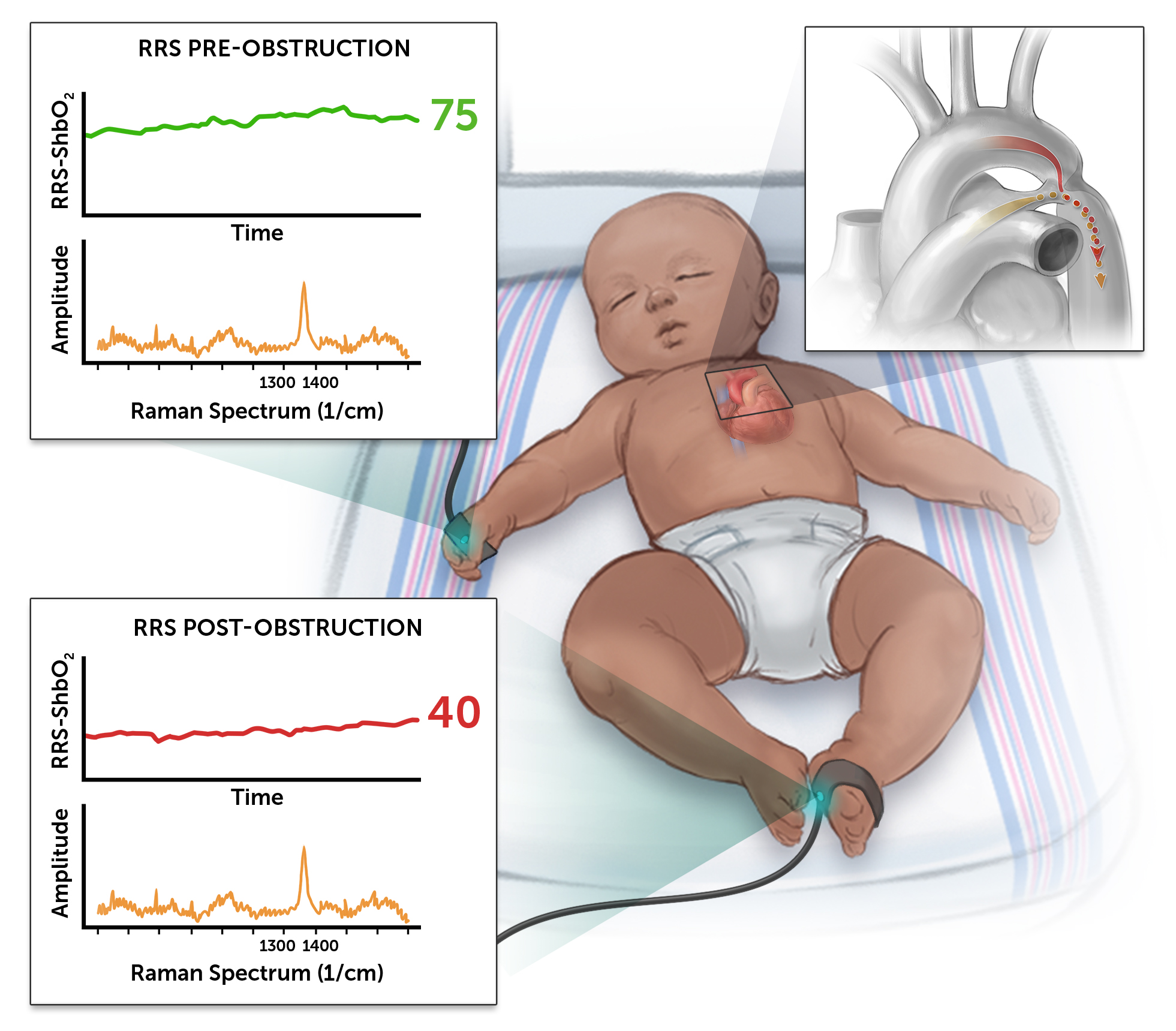 Figure 1. Illustration of infant with RRS probes in place on superficial skin of right palm and sole of foot, showing example pre- and post-ductal RRS values with ductal restriction in the setting of an evolving CoA.
Figure 1. Illustration of infant with RRS probes in place on superficial skin of right palm and sole of foot, showing example pre- and post-ductal RRS values with ductal restriction in the setting of an evolving CoA. 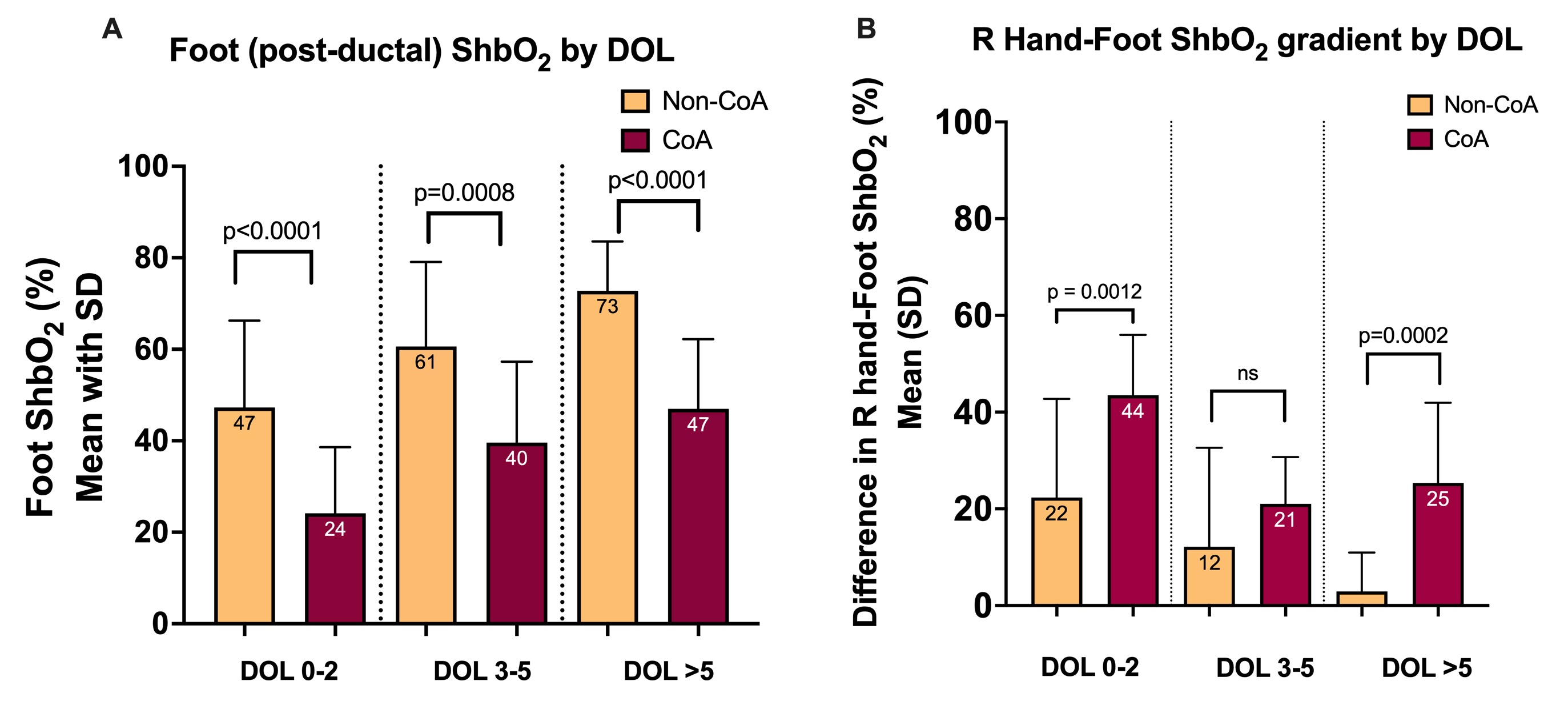 Figure 2A: Mean foot (post-ductal) RRS-ShbO₂ by day of life (DOL) in newborns who did not undergo surgery (non-CoA; yellow) or did undergo surgery (CoA; red). 2B: Pre- (hand) -post-ductal (foot) ShbO₂ gradients by DOL in non-CoA versus CoA group.
Figure 2A: Mean foot (post-ductal) RRS-ShbO₂ by day of life (DOL) in newborns who did not undergo surgery (non-CoA; yellow) or did undergo surgery (CoA; red). 2B: Pre- (hand) -post-ductal (foot) ShbO₂ gradients by DOL in non-CoA versus CoA group. 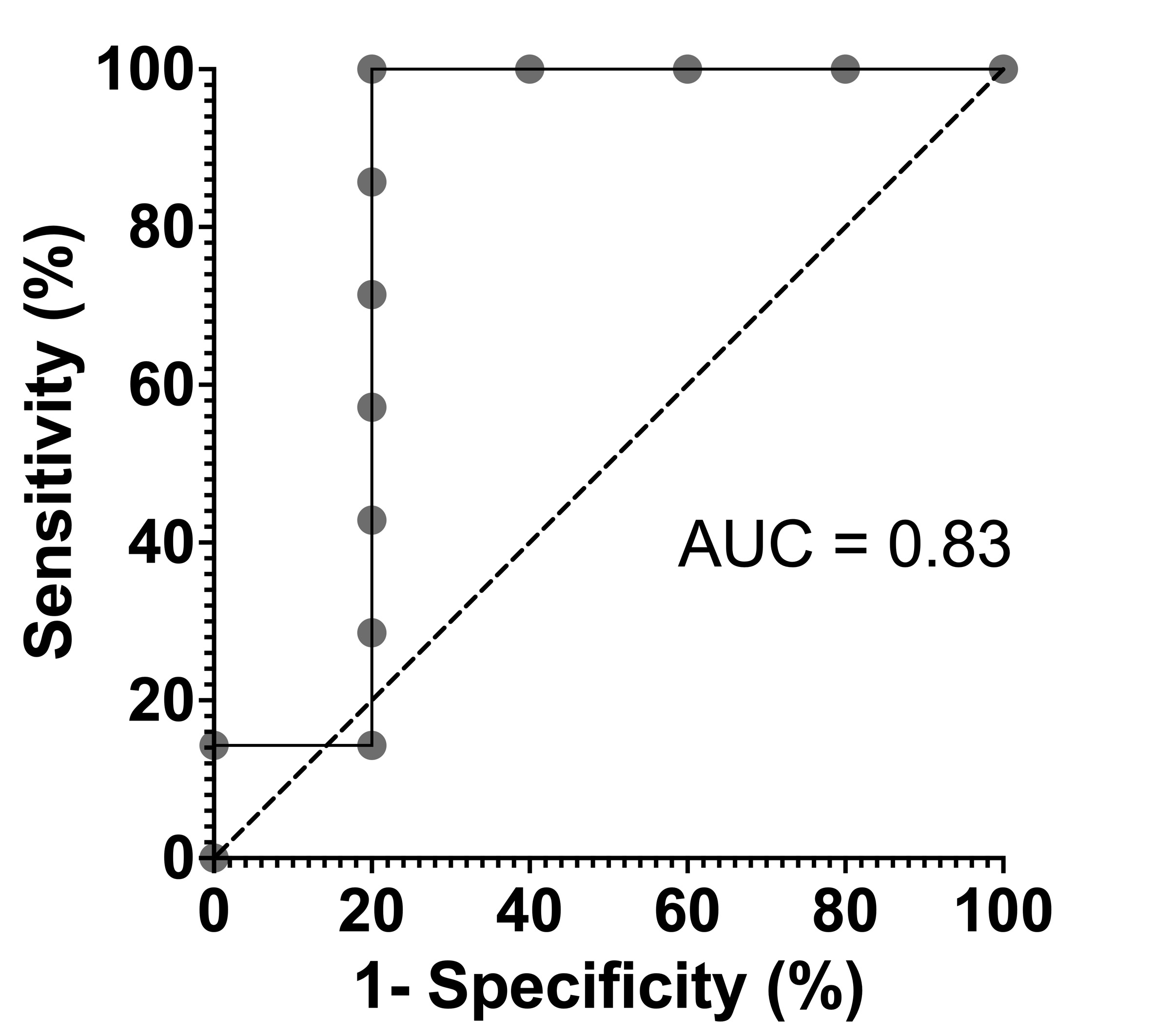 Figure 3. ROC curve showing the predictive performance of patient-level lowest post-ductal (foot) RRS-ShbO₂ on or after day 3 of life for CoA surgery in infants undergoing monitoring for evolving arch obstruction. The threshold of post-ductal RRS-ShbO₂ <39% identified all infants who underwent surgery with 100% sensitivity and 80% specificity (AUC = 0.83).
Figure 3. ROC curve showing the predictive performance of patient-level lowest post-ductal (foot) RRS-ShbO₂ on or after day 3 of life for CoA surgery in infants undergoing monitoring for evolving arch obstruction. The threshold of post-ductal RRS-ShbO₂ <39% identified all infants who underwent surgery with 100% sensitivity and 80% specificity (AUC = 0.83).