350 - Navigating Rural Pediatric Care: A Multi-Site Longitudinal Qualitative Study of Clinician Perspectives and Adaptive Strategies
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4343.350
Jessica D. Jones, Seattle Children's, Bellevue, WA, United States; Tracy J. Yang, University of Washington, Seattle Children's Hospital, Seattle, WA, United States; Emily A. Hall, University of Montana, Big Arm, MT, United States; Corrie E. McDaniel, University of Washington / Seattle Children's Hospital, Seattle, WA, United States
Pediatric Hospital Medicine Fellow Seattle Children's Bellevue, Washington, United States
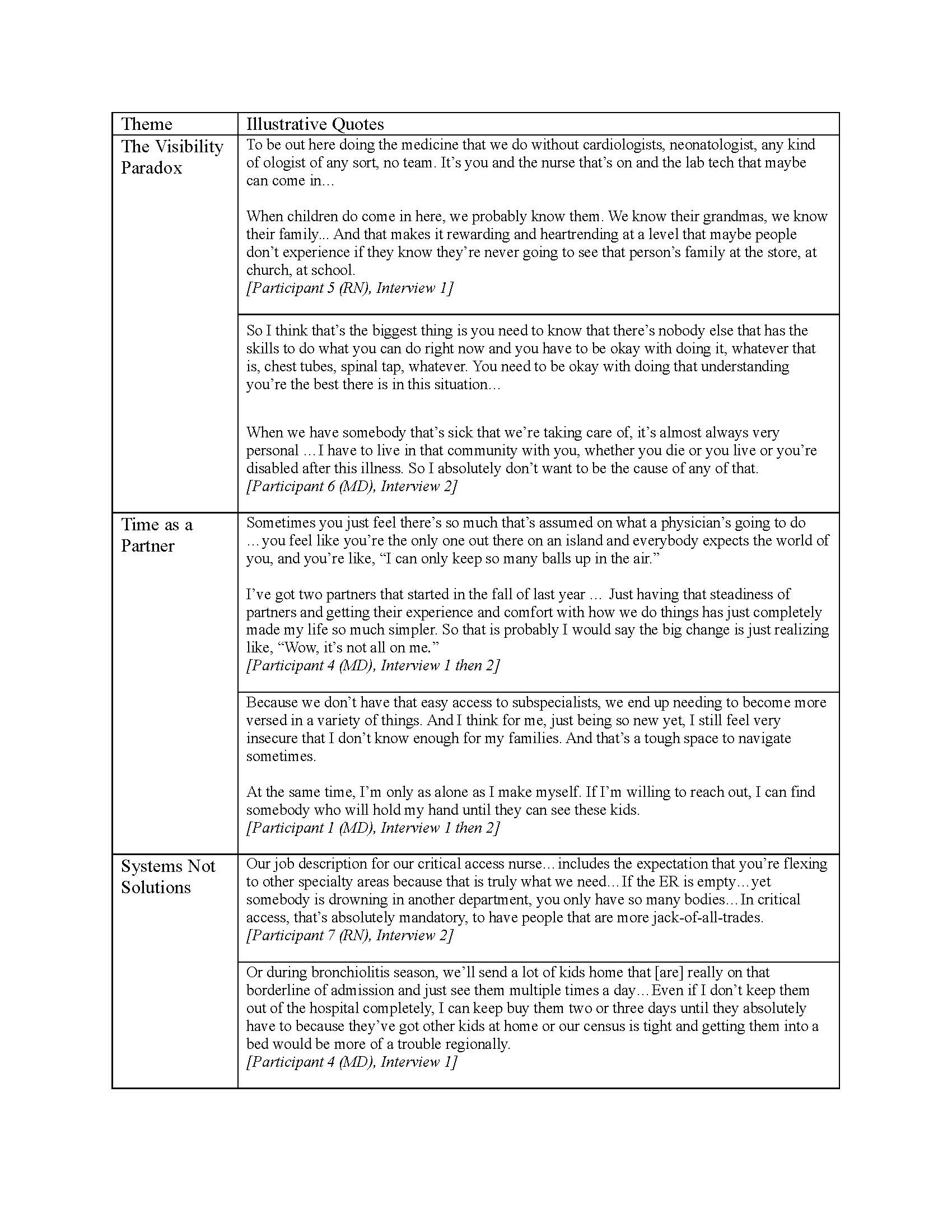
Background: Regionalization of pediatric care has widened healthcare disparities for rural children. Rural clinicians mitigate disparities by providing care locally in resource-constrained hospitals; however, sustaining clinicians in rural practice remains a significant challenge. Little is known about the factors that shape successful rural pediatric practice through time. Objective: We aimed to (1) describe how rural clinicians navigate providing pediatric acute care in resource-limited settings, (2) examine how rural pediatric acute care evolves based on cumulative experiences and changing contextual demands through time. Design/Methods: Our longitudinal qualitative study used purposeful sampling to recruit 9 rural clinicians (5 MDs, 4 RNs) representing 4 hospitals, 3 states (WA, MT, SD), clinical experience 1-42 years (median 25). Three of four hospitals were critical access (median distance to referral center: 179 miles). We conducted semi-structured, iterative interviews with each participant every 6-9 months for a total of 27 interviews (median 59 minutes, range 43-86). Interviews explored how resource navigation and professional relationships evolved through time. We used thematic analysis to identify initial codes and themes through time with a hybrid inductive-deductive approach using complex adaptive systems theory as a conceptual lens. Results: We identified three themes (Table 1): (1) Visibility Paradox: Rural clinicians cope with high-stakes decisions and professional isolation while navigating a high-visibility role in their community. Clinicians noted that the intensity of constant visibility and responsibility makes rural practice difficult to sustain. (2) Time as a Partner: Rural practice relies on the building of local knowledge and relationships bridging time, institutions, roles, and specialties. Clinicians emphasized that, across time, the accumulation of trust and networks made challenges feel more achievable. (3) Systems Not Solutions: In the setting of professional isolation and limited care options, rural clinicians cultivate local systems of care for children that capitalize on unique strengths within a rural setting. Clinicians described moving beyond reactive problem-solving toward intentionally redesigning local systems that harness existing resources to make care sustainable.
Conclusion(s): Our findings capture sophisticated adaptive strategies and systems-level innovations within rural pediatric practice across time. These findings challenge deficit-based narratives about rural healthcare and may inform future interventions that aim to foster sustainable pediatric care in rural areas.
Table 1. Themes illustrating rural clinicians' evolving perspectives on pediatric acute care

 photo")