328 - Earlier speech therapy is associated with decreased length of NICU stay in preterm infants <28 weeks of birth gestational age.
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4322.328
Amanda Mosher, Wake Forest School of Medicine of Wake Forest Baptist Medical Center, Winston-Salem, NC, United States; Kaylee N. Freid, Wake Forest School of Medicine of Wake Forest Baptist Medical Center, Winston-Salem, NC, United States; Jessica P. Walker, Atrium Health Wake Forest Baptist Health, Advance, NC, United States; Peter J. Porcelli, Wake Forest School of Medicine of Wake Forest Baptist Medical Center, Winston-Salem, NC, United States; Jennifer Check, Wake Forest School of Medicine of Wake Forest Baptist Medical Center, Winston-Salem, NC, United States; Parvesh Garg, Wake Forest School of Medicine of Wake Forest Baptist Medical Center, Winston Salem, NC, United States
Medical Student Wake Forest School of Medicine of Wake Forest Baptist Medical Center Winston-Salem, North Carolina, United States
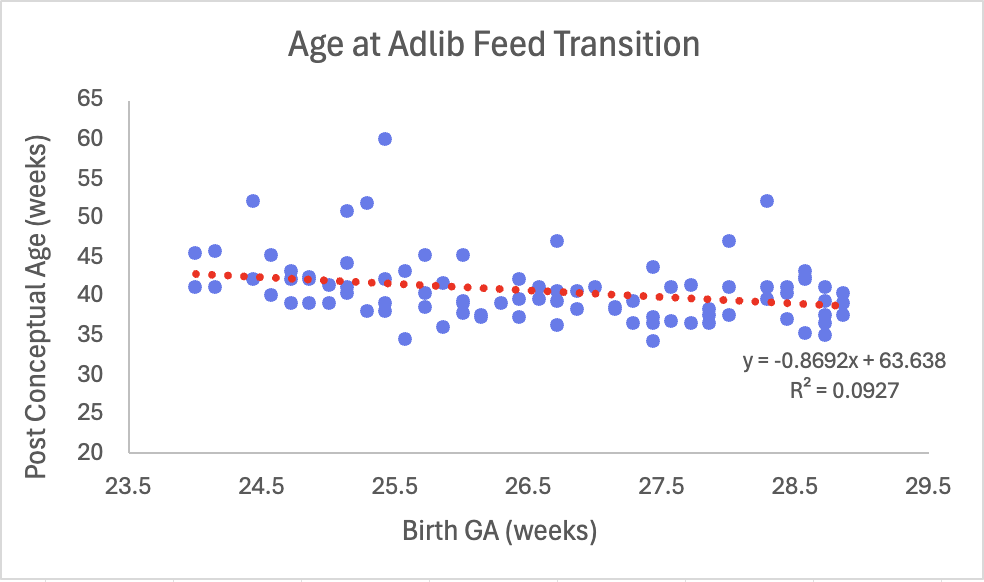
Background: Extremely low gestational age newborns (ELGAN, ≤28 weeks) are at risk for systemic morbidities that impact length of hospital stay and long-term clinical outcomes. Nutritional support is critical for the growth and development of preterm infants. Objective: We compared early ( < 40 week) vs. late (≥40 week) consultation for speech therapy (ST) for feeding difficulties in ELGAN and their long-term outcomes to describe the clinical impact of ST at different post-conceptual ages (PCA). Design/Methods: Infants with a birth GA of 24-28 weeks who received ST from 2022-2024 were enrolled retrospectively. A regression comparing birth GA to post conceptual age at adlib feed transition determined two cohorts. R-software was used to compare clinical outcomes between the cohorts and p-value < 0.05 was considered significant. Results: 84 infants received ST < 40 weeks PCA (group A) compared to 31 infants ≥40 weeks PCA (group B). At time of first visit, group A infants were more often tube fed than group B (94.0% vs 77.4%, p< 0.01). Comorbidities such as bronchopulmonary dysplasia and intraventricular hemorrhage were associated with later age at first ST visit (42.9% group A vs. 58.1% group B, p< 0.01). Though not significant, there was a trend toward infants at lower GA at birth reaching adlib status later than infants born at higher GA (Figure). Group B had significantly higher mean number of occupational therapy (OT) and ST visits during their hospital stay (13.2 vs 20.7 OT; 11.6 vs 18.2 ST, p< 0.01). Group A had higher rates of milk penetration (76.7% vs. 50% p< 0.01) and 2:1 consistency laryngeal penetration (10% vs. 0% p< 0.01). Group B had higher rates of laryngeal penetration at 1:1 consistency (58.3% vs. 20% p< 0.01) and aspiration at 1:2 consistency (90% vs. 64.3% p< 0.01). Group B had a longer mean length of hospital stay (85.8 ± 42.4 days vs 106.0 ± 70.5 days, p=0.05). While no significant difference in tube-feeding at discharge, at 6- and 12-month follow up, group B was tube fed more often than those in group A (10.3% vs 41.4%, p< 0.01 at 6 months, 21% vs 66.7%, p< 0.01 at 12-months). There was no significant difference in Ages and Stages Questionnaire scores at 6 months.
Conclusion(s): Group B was at higher risk of aspiration and laryngeal penetration with higher consistencies (1:1 and 2:1), had higher rates of comorbidities during their NICU stay and required longer LOS. Infants in group B required more therapy, which may be due to the delay in initiation of ST. While group A required more tube feeding initially, they achieved earlier oral feeding at 6- and 12-month long-term follow up compared to group B.

 photo")
.png)