Session: Health Equity/Social Determinants of Health 6
5 - TEAM UP for Equity, an Approach to Improving Behavioral Healthcare Outcomes Using Race, Ethnicity, and Language Data
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4004.5
Destiny Tolliver, Boston University School of Medicine, Boston, MA, United States; Radley C. Sheldrick, UMass Chan Medical School, Shrewsbury, MA, United States; Sonia Erlich, Boston Medical Center, Roslindale, MA, United States; Elijah E. Boliver, Boston Medical Center, Boston, MA, United States; Charlotte Vieira, Boston Medical Center, Concord, MA, United States; Anita Morris, Boston Medical Center, Boston, MA, United States; Emily Feinberg, Hassenfeld Child Health Institute, Brown University School of Public Health, Providence, RI, United States
Assistant Professor Boston University School of Medicine Boston, Massachusetts, United States
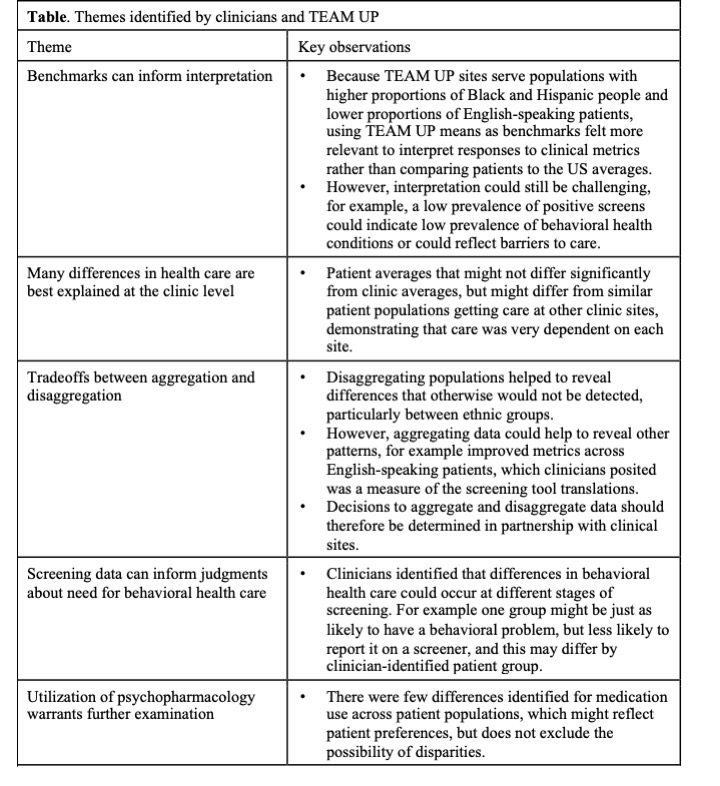
Background: TEAM UP is an evidence-based clinical model that integrates comprehensive behavioral health services into primary care, with an explicit goal to improve health equity. To reduce healthcare disparities, it is necessary to understand health outcomes across patient populations. Race, ethnicity, and language (REL) data have been used to identify patient groups, but traditional categories (e.g., "non-Hispanic White", "non-Hispanic Black") are unable to distinguish nuanced differences to inform interventions. Objective: To develop a novel, clinician-engaged approach to guide and interpret quantitative data analysis regarding health disparities. Design/Methods: The TEAM UP for Equity approach was implemented at 4 Federally Qualified Health Centers. It included four steps: 1) identify health outcomes to prioritize, (e.g., % of population with a positive result on a screening tool, and % identified with a behavioral health problem); 2) engage with clinicians at each site to identify clinically-relevant, mutually-exclusive patient populations (e.g., "Vietnamese families", "Haitian Creole-speaking families"); 3) conduct logistic regression with patient population as the exposure, each health outcome as the dependent variable, and clinical site mean as the reference group; and 4) discuss results with clinicians to clarify differences between statistical and clinical significance and identify areas for improvement. Results: Each site identified 5-7 patient populations. Compared to standard REL variables, the TEAM UP approach identified more statistically significant differences. For example, 11% of REL variables tested using a traditional approach were associated with poorer health outcomes, while 6% were associated with improved outcomes. In contrast, 27% of clinician-identified patient populations tested using the TEAM UP approach were associated with poorer health outcomes, while 18% were associated with improved outcomes. Discussions with site-based clinicians (Table) noted that findings for some race categories differed by culture; for example, whether patients who identified as Black race were more or less likely to screen positive and be identified with a behavioral health problem was contingent on ethnic background (Figure).
Conclusion(s): TEAM UP for Equity is a novel and important approach to identify healthcare disparities and may identify nuanced differences that are often obscured by commonly used REL categories. Systematically incorporating clinician perspectives into data analysis may provide new avenues for conducting health equity research.
Table. Themes identified by clinicians and TEAM UP
Figure. Behavioral healthcare metrics for Black/African-American patients: overall and stratified by language PAS Figure - TU for equity.jpeg

 photo")