397 - Improving Time to Second Opioid Administration in Patients With Sickle Cell Disease Presenting With Vasoocculsive Crisis
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4389.397
Bilal Ahmed, Cohen Children's Medical Center, East Meadow, NY, United States; Kristy Williamson, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Garden City, NY, United States; Kimberly Kahne, Cohen Children's Medical Center, New Hyde park, NY, United States; Joshua Rocker, Cohen Children's Medical Center, New Hyde Park, NY, United States; Isabella Yu, Cohen Children's Medical Center, New Hyde Park, NY, United States; Tabetha Garver-mosher, Northwell Health, New York, NY, United States; Ryan Hardardt, Cohen Children's Medical Center, New Hyde Park, NY, United States; Laura LaMaina, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, New Hyde Park, NY, United States; Gia Aslanidis, Cohen Children's Medical Center, Port Jefferson Station, NY, United States; Kimberly A. Giusto, Northwell Health, rockville centre, NY, United States
Resident Cohen Children's Medical Center East Meadow, New York, United States
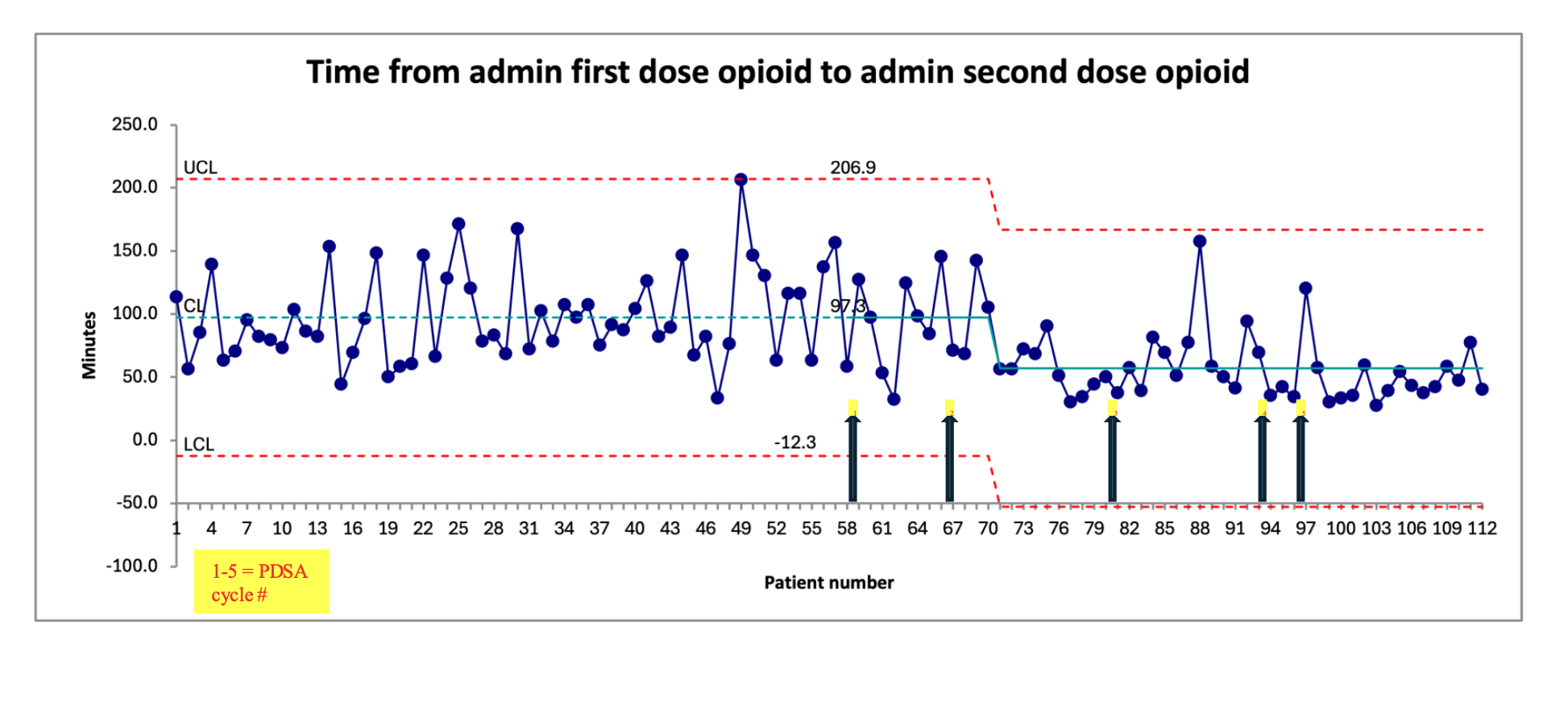
Background: Children with sickle cell disease (SCD) frequently present with vaso-occlusive crises (VOC) requiring timely opioid dosing. Guidelines recommend a second dose within 30 to 60 minutes if pain persists, yet adherence in pediatric emergency departments (PED) remains limited (Rees et al., 2022; Gwarzo et al., 2025). Delays in second dosing are associated with increased hospitalization and inadequately managed pain (Muslu et al., 2020). Objective: Our aim was to decrease mean time from first to second opioid dose in patients with SCD presenting to the PED with VOC by 40% by 9/30/25. Design/Methods: Using quality improvement methodology, a multi-disciplinary group at an urban PED met to improve time to second dose of opioid in SCD patients presenting with VOC. A retrospective analysis was performed to establish baseline data. During PDSA 1, education efforts were targeted to nurses and physicians (attendings/fellows) through newsletters, e-mails, departmental meetings, and bedside teaching. Education on timeliness, dosing, and guidelines was presented to residents in pediatrics (PDSA 2) and emergency medicine (PDSA 3). In PDSA 4, we introduced the ability to order the second dose of opioid PRN concurrently with the first dose so the primary nurse can activate independently. PDSA 5 involved signage on PED computers with reminders regarding the new process. Patients were excluded if they only received one dose of opioid, greater than 150 minutes lapsed from administration of the first dose to the order of second dose, or the patient had a documented pain reassessment of < 5 after the initial dose. The primary outcome was time from administration of first opioid dose to administration of second dose in patients with SCD and continued moderate to severe pain. Results: Pre-data (9/1/24 to 3/31/25) included 58 patients with a mean time to second opioid dose of 97 minutes. The intervention phase (4/1/25 to 9/19/25) included 54 patients with a mean time to second opioid dose of 65 minutes (45 minutes by PDSA 5, a 46% reduction). We had a centerline shift in the desired direction which was sustained throughout the project with a trend toward a second shift. We saw an 18% decrease in admission rate during the intervention phase. We did not see any difference in mean total opioid dose per kg per visit during intervention phase compared to pre data.
Conclusion(s): Multidisciplinary education, structured reassessment, streamlined order input, and physical reminders significantly improved adherence to timely second dose opioid administration in pediatric SCD crises.
Time from admin first dose opioid to admin second dose opioid

 Credit")