358 - Association of Patient Portal Enrollment and Use with Inpatient Hospitalization Outcomes
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4351.358
Yinlu Zhu, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, United States; Courtney Wolk, University of Pennsylvania, Philadelphia, PA, United States; Stephanie G. Menko, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Danielle Capriola, Childrens Hospital of Philadelphia, Sanatoga, PA, United States; Kate M.. Fuller, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Philip Scribano, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Chris Bonafide, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Aditi Vasan, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Michael J. Luke, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Medical Student Perelman School of Medicine at the University of Pennsylvania Philadelphia, Pennsylvania, United States
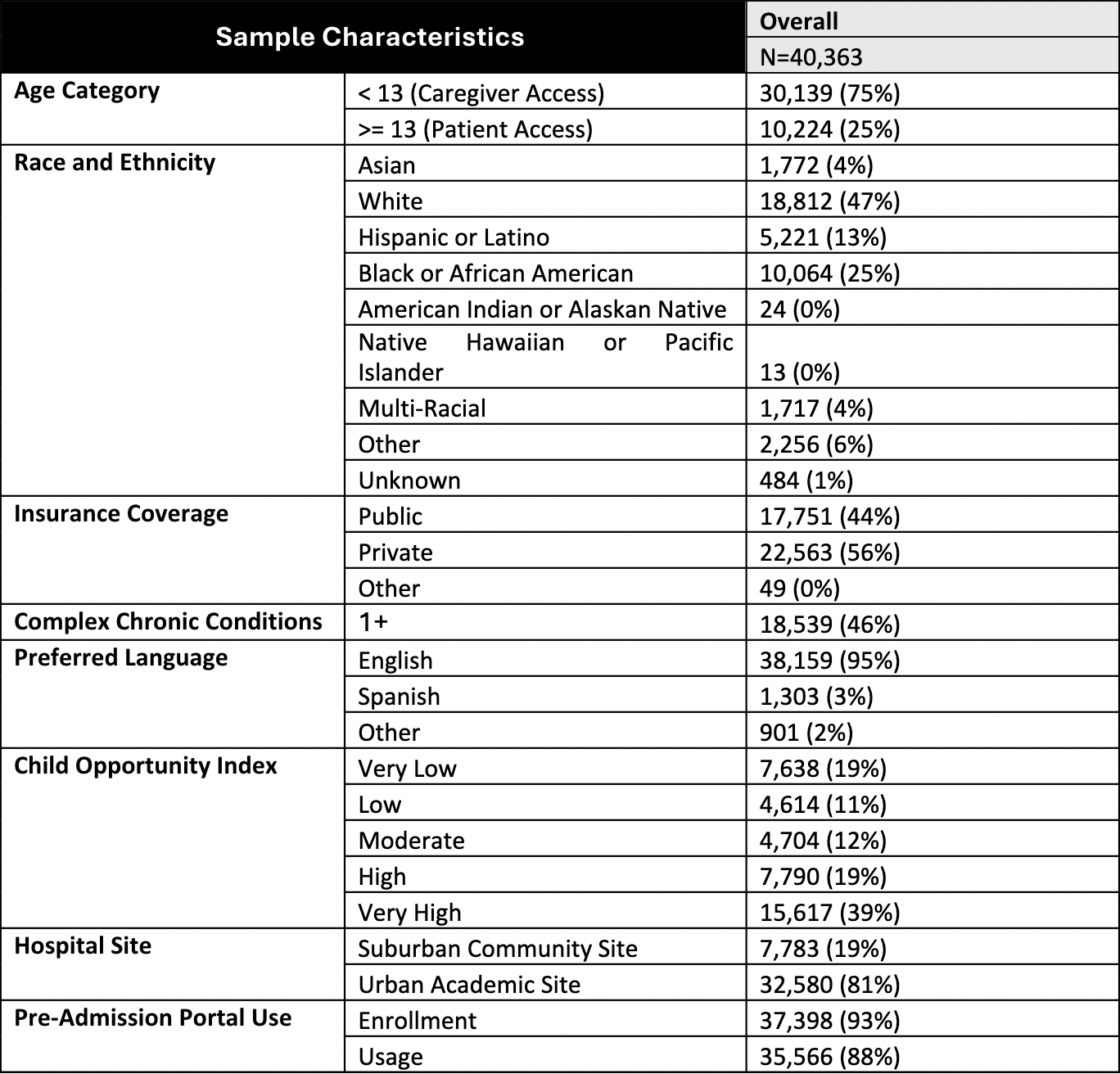
Background: Patient portals enable patients and caregivers to better access health information, actively engage with preventative care, and make more informed health decisions. It remains unclear how portal enrollment and portal use impact care utilization, particularly among hospitalized children, who often represent a high-risk population with greater health care needs. Objective: To evaluate the association between patient portal enrollment and use and hospitalization outcomes, including (1) admission to a critical care unit, (2) length of stay (LOS), and (3) readmissions within 6 months following discharge. Design/Methods: This cross-sectional study included 40,363 children hospitalized at either an urban quaternary or a suburban tertiary care children's hospital within a single health system between 2022 and 2024. We defined portal enrollment as enrollment status at admission and portal use as any login, message sent, or telehealth encounter in the 12 months prior to admission. We used multivariable logistic regression to examine associations between portal enrollment and use and critical care admission, adjusted for age, race/ethnicity, neighborhood opportunity, insurance status, primary language, and medical complexity, with time and site fixed effects. We used multivariable negative binomial regression to examine associations between portal enrollment and use and hospital LOS and readmissions, controlling for admitting service in addition to the aforementioned covariates. Results: Among 40,363 patients (Table 1), the 93% of patients with prior portal enrollment (OR 0.68, CI 0.61-0.76) and the 88% of patients with prior portal use (OR 0.64, CI 0.58-0.70) had significantly lower odds of critical care admission (Figure 1). Patients with prior portal enrollment (IRR 0.68, CI 0.63-0.74) and use (IRR 0.74, CI 0.69-0.80) also had significantly shorter LOS. Portal enrollment was not associated with readmissions (IRR 0.96, CI 0.88-1.06), but portal use was associated with increased incidence of readmissions (IRR 1.12, CI 1.02-1.22) (Figure 2).
Conclusion(s): Patient portal use was associated with shorter lengths of stay and a lower likelihood of admission to critical care, which could be attributed to more prompt recognition of acute illness and presentation to care. Active patient portal users were also more likely to experience readmissions, which could indicate increased medical complexity, a lower threshold to seek care, or more prompt detection of post-discharge problems warranting reassessment. Future research should explore the indications for these readmissions.
Table 1: Patient Characteristics
Figure 1. Odds of Critical Care Admissions with Portal Enrollment/Use
Figure 2. Incidence Rates of Longer LOS and Readmissions with Portal Enrollment/Use

 photo")
.png)
.png)
