542 - Hypogammaglobulinemia and B cell repopulation after rituximab treatment in childhood nephrotic syndrome
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4530.542
Cal H. Robinson, The Hospital for Sick Children, Toronto, ON, Canada; Nowrin Aman, The Hospital for Sick Children, Toronto, ON, Canada; Josefina A. Brooke, the Hospital for Sick Children, Toronto, ON, Canada; Valentina Bruno, The Hospital for Sick Children, University of Toronto, Toronto, ON, Canada; Vaneet Dhillon, The Hospital for Sick Children, Toronto, ON, Canada; Mackenzie Garner, The Hospital for Sick Children, Toronto, ON, Canada; Christoph Licht, The Hospital for Sick Children, Toronto, ON, Canada; Seetha Radhakrishnan, The Hospital for Sick Children, Toronto, ON, Canada; Keisha Rasool, The Hospital for Sick Children, Toronto, ON, Canada; Nithiakishna Selvathesan, The Hospital for Sick Children, Toronto, ON, Canada; Chia Wei Teoh, The Hospital for Sick Children, Toronto, ON, Canada; Jovanka Z. Vasilevska, The Hospital for Sick Children, Toronto, ON, Canada; Rulan Parekh, Women's College Hospital, Toronto, ON, Canada
Pediatric Nephrologist The Hospital for Sick Children Toronto, Ontario, Canada
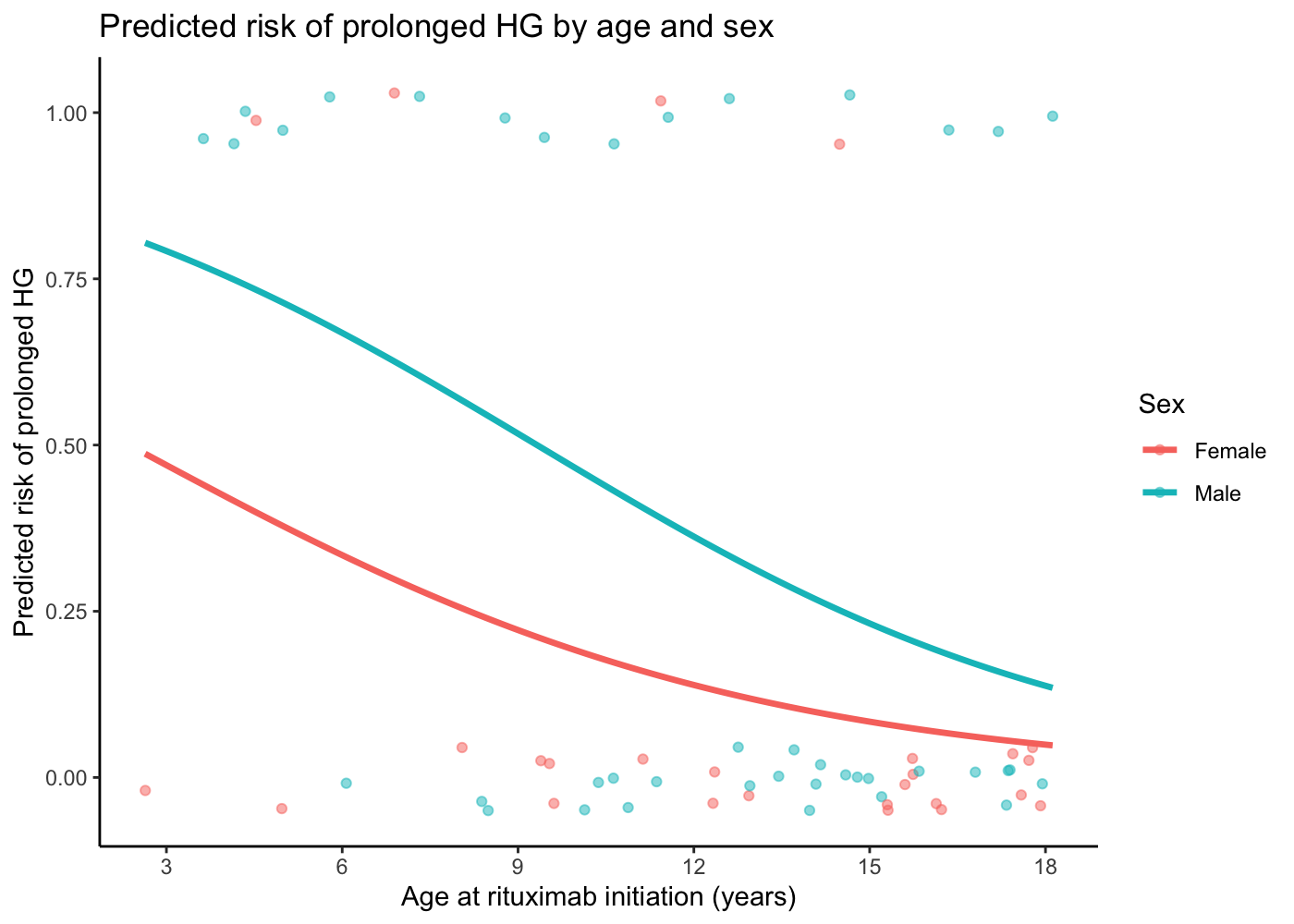
Background: Rituximab is commonly used to treat children with steroid-resistant and frequently-relapsing nephrotic syndrome. Although rituximab effectively induces remission and prevents relapses, its long-term safety in children with nephrotic syndrome is poorly understood. Objective: Our aims were to evaluate the incidence and risk factors for hypogammaglobulinemia, hematological complications, B cell repopulation, and relapses after rituximab treatment. Design/Methods: We included children (1-18 years) with nephrotic syndrome that were enrolled in a prospective cohort study (Greater Toronto Area, Canada) and received rituximab treatment from Jun 2018 to Dec 2023. We collected all immunoglobulin, hematology, and microbiology test results performed at our institution. The primary outcome was hypogammaglobulinemia (IgG < 5g/L), classified as severe (IgG < 3g/L) and/or prolonged (IgG < 5g/L for ≥9-months). Secondary outcomes included other immunoglobulin and hematological parameters, B cell depletion, B cell repopulation, and relapses. Results: Seventy children with nephrotic syndrome received rituximab and had complete laboratory data during our study period. Pre-existing hypogammaglobulinemia was present in 30% of children at rituximab initiation. Hypogammaglobulinemia occurred after rituximab treatment in 55% of children. Of these, 58% had severe and 53% had prolonged hypogammaglobulinemia. Younger age and lower pre-treatment IgG levels were significant risk factors for prolonged hypogammaglobulinemia post-rituximab. After rituximab treatment, 16% of children had anemia, 21% had neutropenia, and 3% had thrombocytopenia. Twelve children (17%) developed documented infections. All children experienced complete B cell depletion by 3-months post-rituximab. Receiving a ≥2-dose rituximab course was associated with longer B cell depletion (p < 0.001), but no difference in time-to-relapse (p=0.24). Time-to-relapse was longer in children that received maintenance immunosuppression vs. did not (p=0.05).
Conclusion(s): Prolonged hypogammaglobulinemia is common post-rituximab in children with nephrotic syndrome. Younger children and lower pre-treatment IgG increase the risk of prolonged hypogammaglobulinemia. Serious infections and other hematological complications are uncommon.
Predicted risk of prolonged hypogammaglobulinemia (HG) by age at rituximab initiation and sex