103 - Reducing Early Readmissions after Neonatal Intensive Care Unit Discharge: A Quality Improvement Project
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3099.103
Doron Kahn, Joe DiMaggio Children's Hospital at Memorial Regional Hospital, Hollywood, FL, United States; Claire Barrette, Joe DiMaggio Children's Hospital at Memorial Regional Hospital, Hollywood, FL, United States; Ilyse Richman, Joe DiMaggio Children's Hospital at Memorial Regional Hospital, Hollywood, FL, United States
Neonatologist Joe DiMaggio Children's Hospital at Memorial Regional Hospital Hollywood, Florida, United States
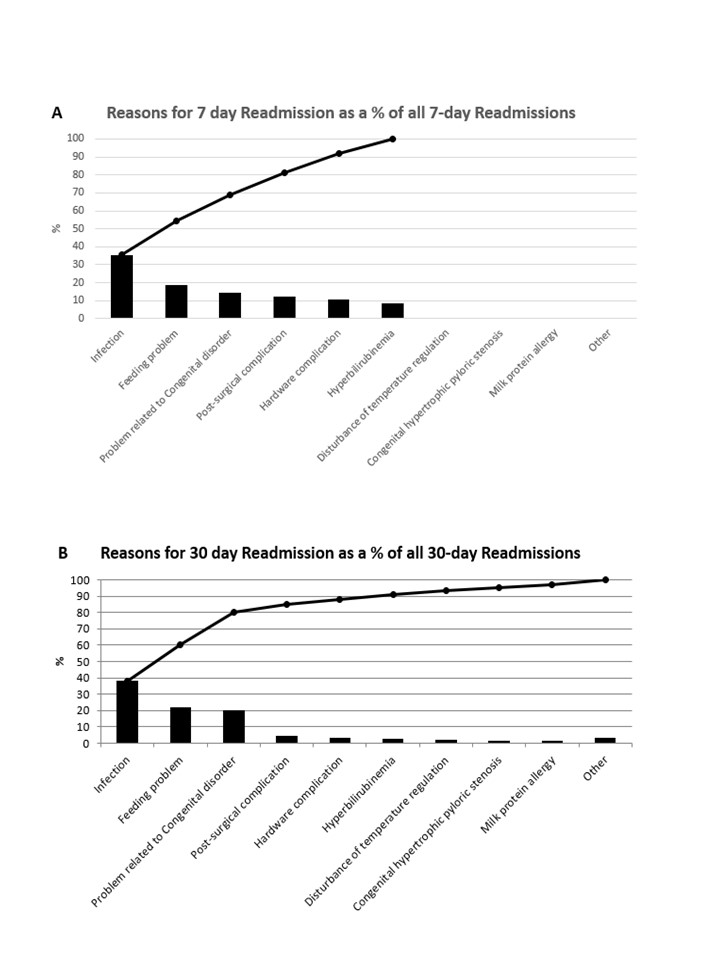
Background: Limited data exists regarding Neonatal Intensive Care Unit (NICU) rates, indications, and evidence for prevention of readmissions. Objective: The purpose of this project was to reduce 7-day and 30-day readmission rates from our baseline to < 1% and < 3%, respectively. We also determined cost savings achieved through reductions in our readmissions. As a balancing measure, we monitored length of stay during initial NICU hospitalization. Design/Methods: We established a QI project using the Model for Improvement focused on readmissions of infants discharged from our level IV NICU. Our SMART aims were to reduce 7-day and 30-day readmission rates from baseline 1.2% and 4.1% to < 1% and < 3%, respectively. PDSA cycles included formation of a readmission team comprised of a neonatologist, nurse practitioner, quality specialist, discharge navigator and parent, review of historical data and monthly readmissions, and presentation of data to providers. Central to the PDSA cycles were development of strategies to avoid readmissions, especially those we deemed preventable, establishment of weekly rounds to assess readiness for discharge, encouraging parents to room in and actively participate in their infant's care, parental education (i.e. keep baby bundled in pediatrician office until doctor in room to prevent hypothermia, demonstration of feed and medication preparation to avoid errors in mixing/administration at home), post-discharge follow-up with caregiver within 24 hours of discharge, and provider-to-community pediatrician communication for high-risk discharges. Results: Readmission rates were lower in 2012-2024 and showed a downward trend downward compared to the baseline period of 2010-2011, with most years exceeding our established goals. (Figure 1 - Data presented annually due to seasonal variation in readmission rates). Infectious etiology followed by feeding-related issues were the most common causes of both 7-day and 30-day readmissions. (Figure 2) Readmissions that we deemed preventable also showed a downward trend over time. Feeding-related issues followed by hyperbilirubinemia were the most common preventable causes of readmission. Cost savings realized through this project totaled $382,773 over 13 years. Despite a successful reduction in readmissions, there was no concomitant increase in length of stay over time.
Conclusion(s): Maintaining a QI project focused on reducing post-NICU discharge readmissions is both feasible and effective. Certain causes, such as feeding-related issues and hyperbilirubinemia, are more amenable to interventions aimed at reducing readmissions.

 Credit")
.jpg)