129 - Pediatric Trainees’ Educational Needs in Shared Decision-Making: Confidence and Learning Preferences within a Competency Framework.
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4126.129
Vanessa Ivonne Orellana Villazon, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Jennifer DeSante-Bertkau, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Ellen Lipstein, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States
Research Fellow Cincinnati Children's Hospital Medical Center Cincinnati, Ohio, United States
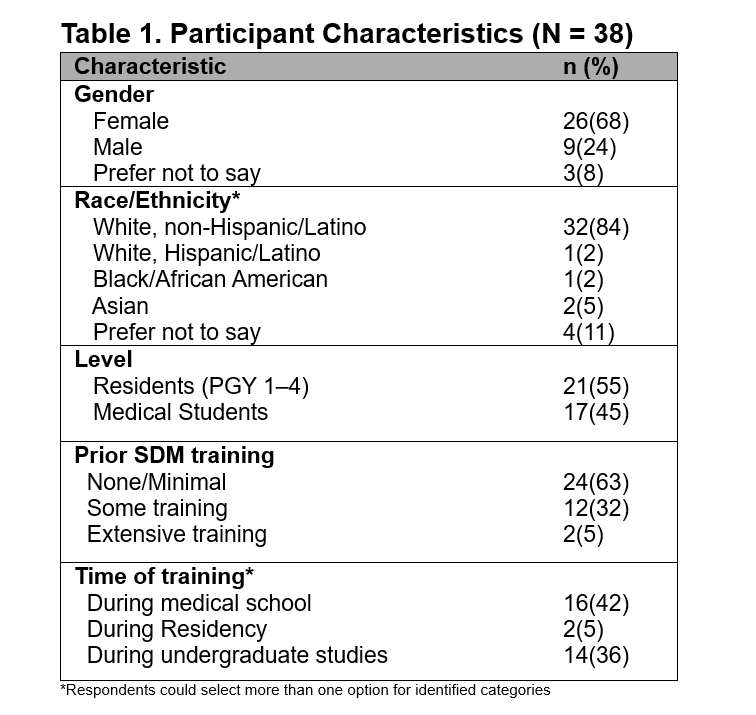
Background: Shared decision-making (SDM) is a core competency in pediatric care, where clinicians, patients, and families work together to make informed choices. Despite its recognized importance, little is known about pediatric trainees' educational needs and learning preferences related to SDM. Evaluating these perceptions through a competency-based lens can clarify how residents develop SDM skills and reveal key educational needs to guide future training. Objective: To assess educational needs regarding pediatric SDM competencies and training among pediatric trainees Design/Methods: We conducted a cross-sectional survey among pediatric residents and senior medical students who reported a strong likelihood of going into pediatrics within an academic quaternary-care children's hospital. The survey drew on a framework of 32 pediatric SDM competencies across six domains, established by expert consensus. Participants rated their confidence in each competency using a four-point scale. Additional items assessed prior SDM training, barriers, and facilitators. Open-ended questions explored participants' understanding of SDM, perceptions of ideal training characteristics, and when SDM education would be most useful. Quantitative data were summarized descriptively; open-ended responses were analyzed thematically. Results: 38 trainees completed the survey (Table 1); 61% reported little or no prior SDM training. Confidence varied across domains: most participants felt confident explaining treatment options to caregivers (82%) but less so involving children (50%). Only 45% felt confident assessing children's readiness to participate, and 26% felt comfortable managing parent-child disagreements. Residents generally reported higher confidence than medical students across most domains, though students showed slightly greater confidence in eliciting children's values. Overall, trainees felt more prepared to communicate with parents than to include children in SDM. Thematic analysis revealed three main themes: (1) SDM was often described as a clinician-parent process, with limited recognition of the child's role; (2) trainees emphasized the need for longitudinal and practice-based SDM learning; and (3) they valued protected time, observation, and feedback opportunities to build confidence.
Conclusion(s): Findings suggest that pediatric trainees do not feel confident about when or how to apply SDM. Effective SDM education should integrate experiential learning throughout residency, emphasize strategies for involving children, and provide structured opportunities for practice and reflection within a competency-based curriculum.