468 - Evidence of Increased Respiratory Morbidity and Pulmonary Vascular Disease in School-Age Children Born Premature
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4459.468
Aimilia Eirini Papathanasiou, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Kimberley G. Miles, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Matthew Willmering, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Nehal A. Parikh, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Erik Hysinger, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Jason Woods, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Paul Critser, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States
Pediatric Resident Cincinnati Children's Hospital Medical Center Cincinnati, Ohio, United States
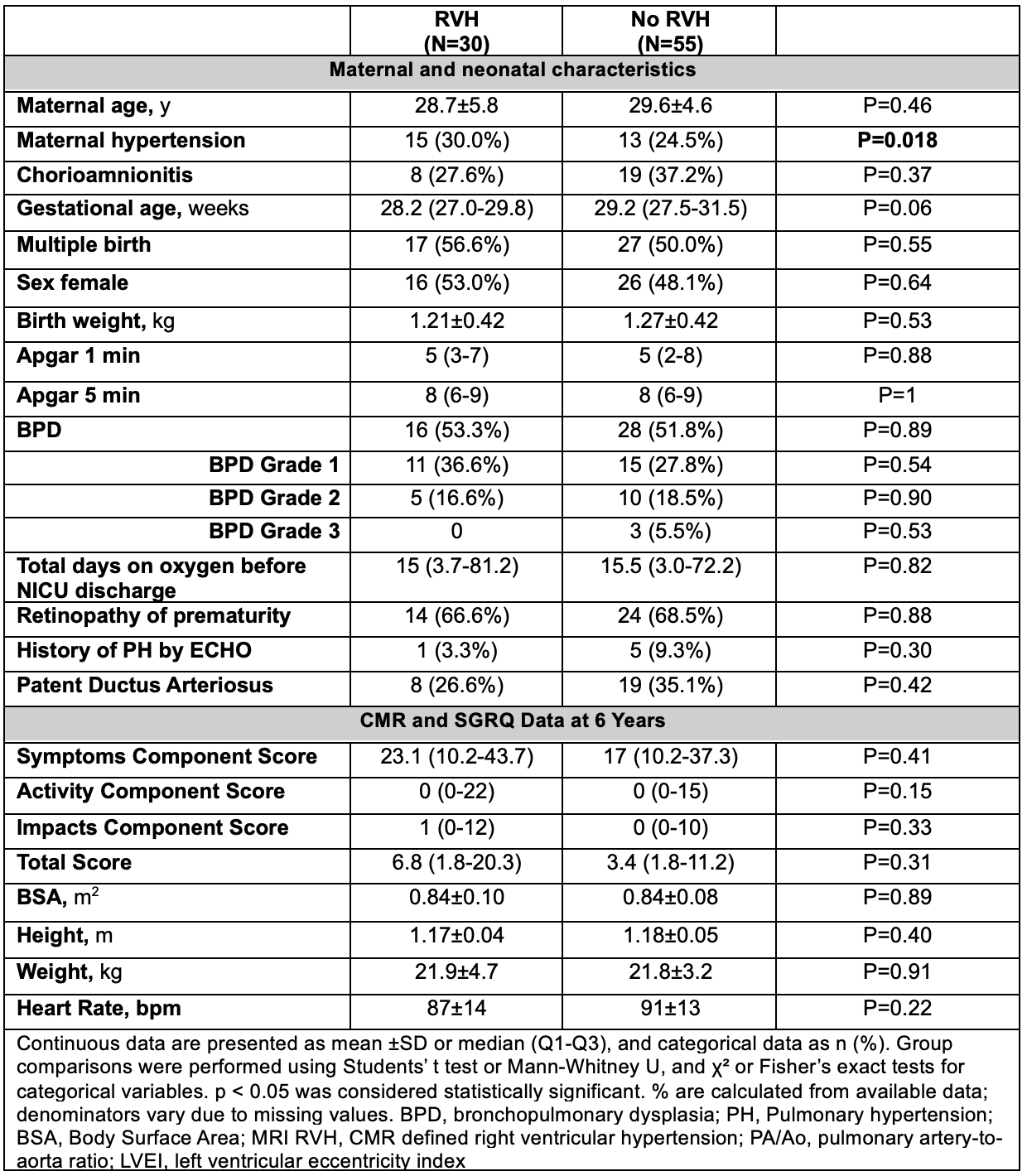
Background: Prematurity remains a leading cause of long-term morbidity. Despite improved survival of preterm infants, young adults born preterm are at increased risk for pulmonary parenchymal and vascular disease. However, the onset of these changes, and the extent to which perinatal factors contribute to this trajectory, remain incompletely understood. Objective: To assess whether school-age children born preterm exhibit evidence of respiratory morbidity and right ventricular hypertension (RVH) compared with healthy term controls and to explore perinatal and neonatal factors associated with this finding. Design/Methods: In this prospective study, preterm children ( < 32 weeks gestational age) from the Cincinnati Infant Neurodevelopment Early Prediction Study cohort and healthy term controls matched for sex, age, and community deprivation index completed SGRQ assessment and underwent cardiac MRI (CMR) at age 6 years on a 3.0 T scanner. Markers of RVH included end-systolic left ventricular eccentricity index (LVEI) >1.15 and pulmonary artery-to-aorta (PA/Ao) ratio >1.1. Respiratory morbidity was evaluated using the St George's Respiratory Questionnaire (SGRQ). Results: Compared with term controls (n=24), preterm children (n=85; mean gestational age 28.9 +/- 2.4 weeks) reported higher SGRQ Activity, Symptoms, Impact, and Total scores (Table 1), reflecting greater respiratory symptoms and functional limitations. Markers of RVH were significantly more common in preterm children (35% vs. 4%, p=0.002), with higher PA/AO ratios (Table 1; Figure 1). RVH was associated with higher SGRQ Activity scores (p = 0.042), however, this association was no longer significant after controlling for prematurity. Among preterm children with RVH, maternal hypertension was the only neonatal or NICU variable independently associated with CMR markers of RVH (p=0.024). Specifically, total days of oxygen, BPD severity, history of PDA, and history of pulmonary hypertension by echocardiography in the neonatal period were not associated with CMR markers of RVH at 6 years of age. Maternal, neonatal, CMR and SGRQ findings stratified by the presence of RVH among preterm participants are presented in Table 2.
Conclusion(s): Preterm birth was associated with CMR markers of RVH, greater respiratory symptom burden, and functional limitation in young school-aged children. Maternal hypertension emerged as a potential perinatal risk factor and merits further investigation. Ongoing longitudinal surveillance is warranted in this at-risk population.
Table 1. Maternal, neonatal, CMR, and St George's Respiratory Questionnaire (SGRQ) characteristics in preterm and term children
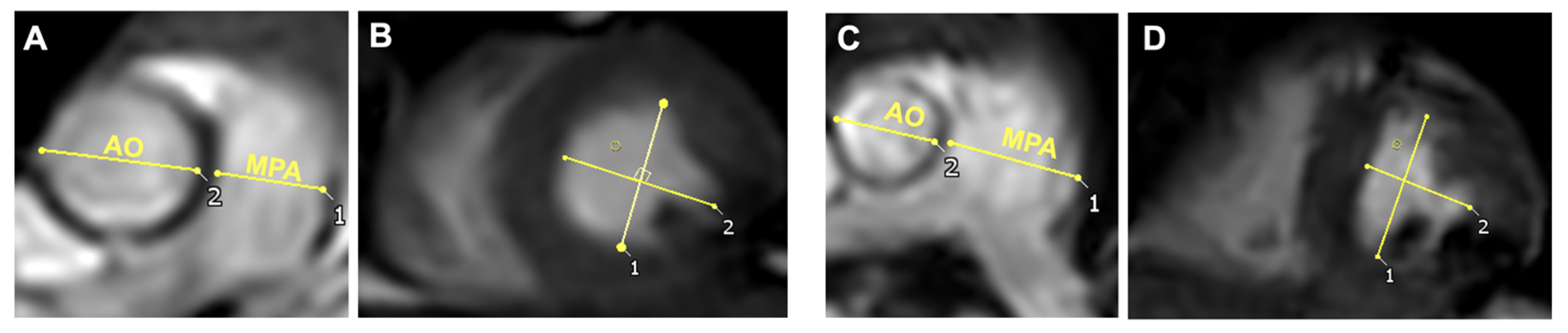
Figure 1. Cardiac MR-derived pulmonary artery-to-aorta (PA/Ao) ratio (A, C) and left ventricular eccentricity index (LVEI) (B, D) in healthy term controls (A, B) and children born preterm (C, D). MR LVEI was determined as the ratio of the LV diameter parallel to the interventricular septum and the diameter perpendicular to the interventricular septum at end systole (B,D)
Table 2. Maternal, neonatal, CMR, and St George's Respiratory Questionnaire (SGRQ) characteristics in preterm children with and without markers of right ventricular hypertension (RVH)


.png)