
Neonatal General
Session: Neonatal General 8: Neurology II

Thomas Hays, MD, PhD
Assistant Professor of Pediatrics
Columbia University Irving Medical Center
Columbia University
New York, New York, United States
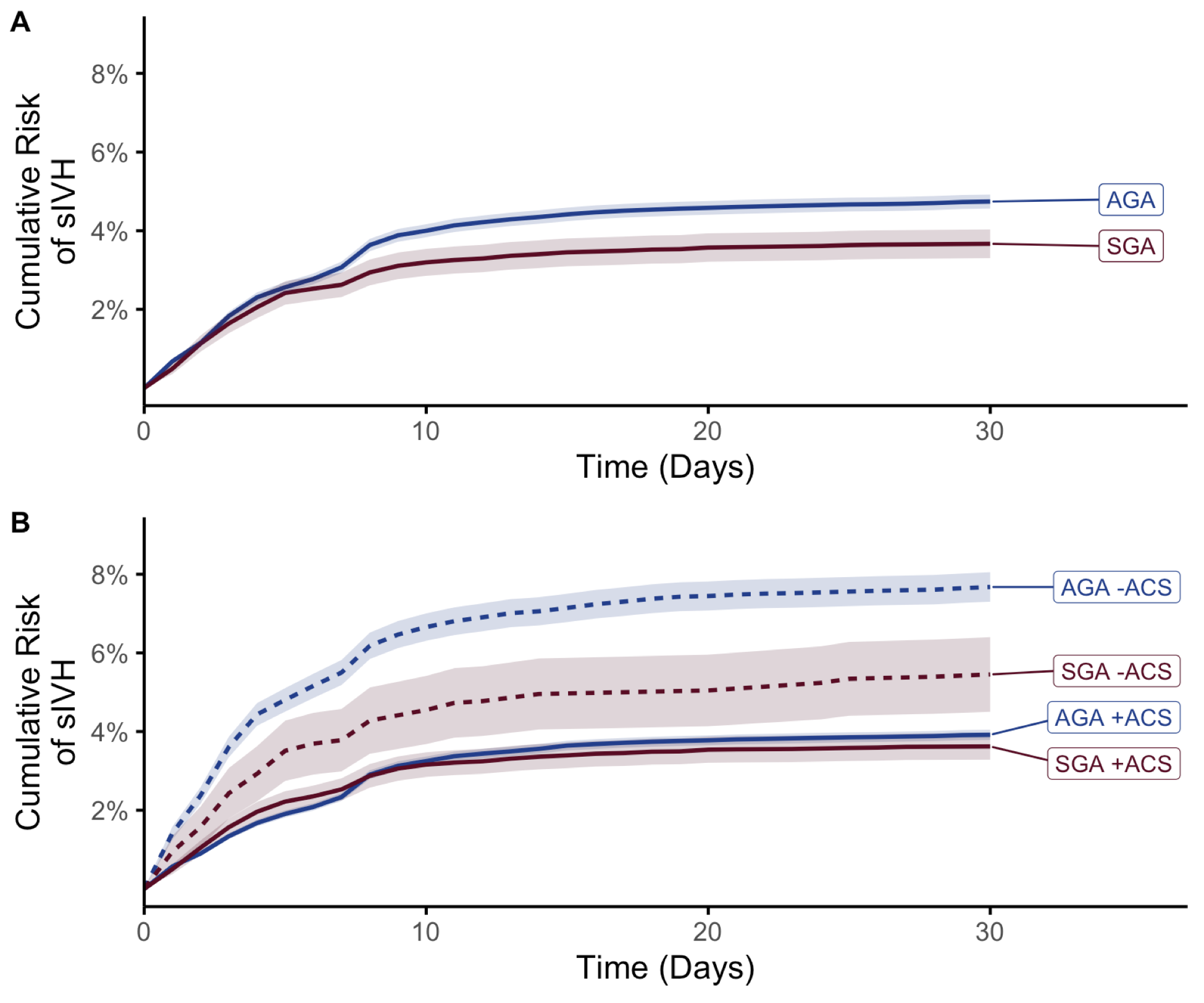 Figure 1. sIVH in a competing risk model accounting for mortality. Infants were grouped by birth weight according to Fenton criteria as small for gestational age or appropriate for gestational age. The risk of sIVH was determined for both groups using a competing risk model, accounting for mortality as a competing outcome, and plotted with 95% confidence intervals. Small for gestational age infants had a lower cumulative risk of sIVH when accounting for mortality as a competing outcome (A). Antenatal corticosteroid exposure was associated with lower cumulative sIVH risk for small for gestational age and appropriate for gestational age infants (B).
Figure 1. sIVH in a competing risk model accounting for mortality. Infants were grouped by birth weight according to Fenton criteria as small for gestational age or appropriate for gestational age. The risk of sIVH was determined for both groups using a competing risk model, accounting for mortality as a competing outcome, and plotted with 95% confidence intervals. Small for gestational age infants had a lower cumulative risk of sIVH when accounting for mortality as a competing outcome (A). Antenatal corticosteroid exposure was associated with lower cumulative sIVH risk for small for gestational age and appropriate for gestational age infants (B). 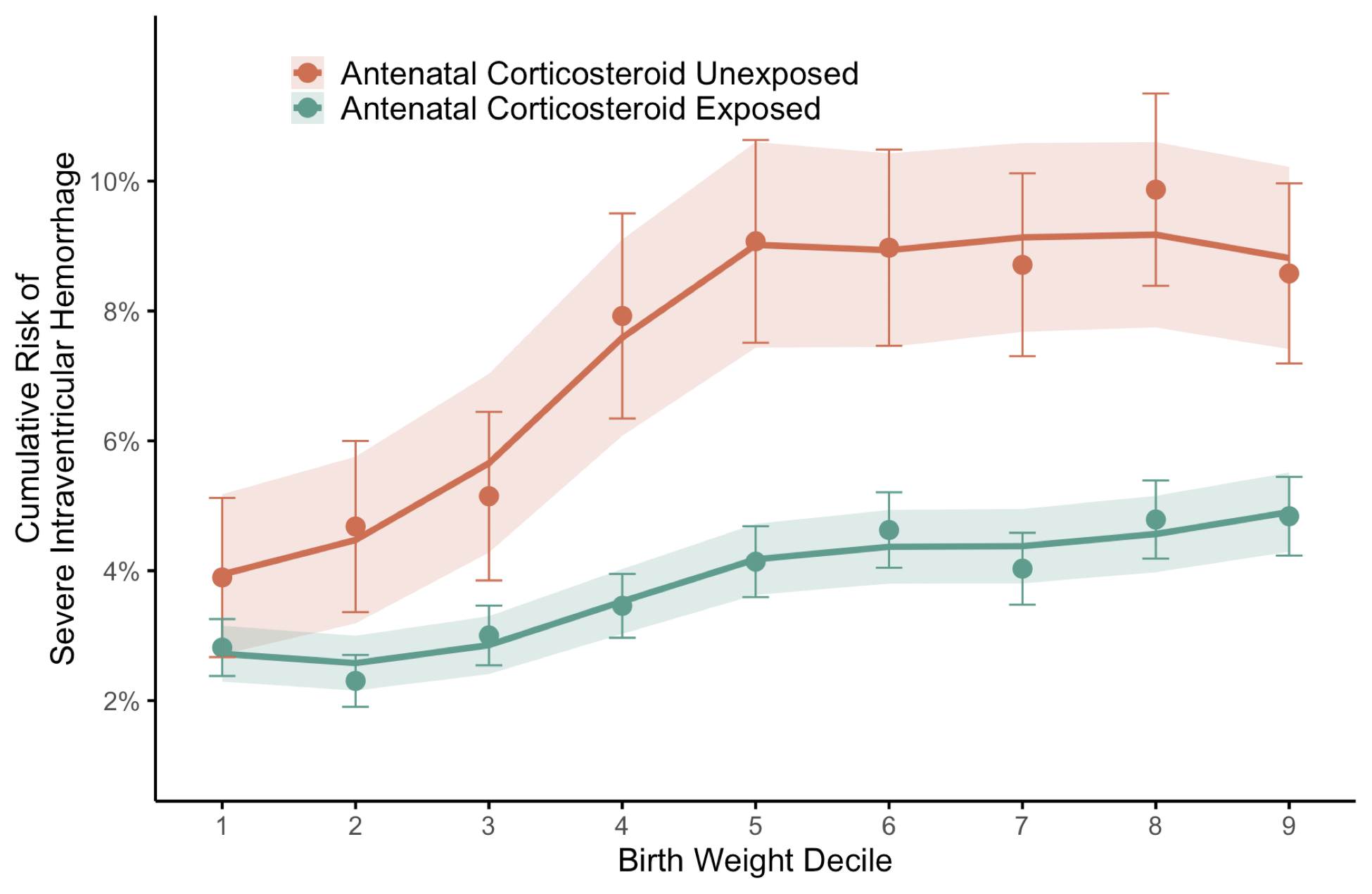 Figure 2. Cumulative risk of severe intraventricular hemorrhage by birth weight decile. The cumulative risk of severe intraventricular hemorrhage at 30 days was determined using a competing risk model, treating mortality as a competing outcome. This risk was determined for infants by birth weight decile (normalized for gestational age and sex). Infants large for gestational age and in the 10th decile were not included in the analysis. Infants were stratified on the basis of exposure to antenatal corticosteroids. Infants in the 1st decile birth weight exhibited the lowest cumulative risk of sIVH, which converged for infants exposed and unexposed to antenatal corticosteroids. Cumulative risk of sIVH increased with greater birth weight decile for infants exposed and unexposed to antenatal corticosteroids, remaining lower for those exposed.
Figure 2. Cumulative risk of severe intraventricular hemorrhage by birth weight decile. The cumulative risk of severe intraventricular hemorrhage at 30 days was determined using a competing risk model, treating mortality as a competing outcome. This risk was determined for infants by birth weight decile (normalized for gestational age and sex). Infants large for gestational age and in the 10th decile were not included in the analysis. Infants were stratified on the basis of exposure to antenatal corticosteroids. Infants in the 1st decile birth weight exhibited the lowest cumulative risk of sIVH, which converged for infants exposed and unexposed to antenatal corticosteroids. Cumulative risk of sIVH increased with greater birth weight decile for infants exposed and unexposed to antenatal corticosteroids, remaining lower for those exposed.