545 - Comparing glomerular filtration rate estimating equations to determine acute kidney injury in children and adolescents with diabetic ketoacidosis
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4533.545
Kelly R.. Bergmann, Children's Minnesota, Minneapolis, MN, United States; Paige Reimche, Children's Hospitals and Clinics of Minnesota, Minneapolis, MN, United States; Amanda J. Nickel, Children's Hospitals and Clinics of Minnesota, Minneapolis, MN, United States; Anupam Kharbanda, Children’s Minnesota, Minneapolis, MN, United States; Catherine Coughlin, Boston Children's Hospital, Boston, MA, United States; Adam Isacoff, University of Louisville School of Medicine, Louisville, KY, United States; Caitlin Valentino, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; David Guernsey, NYU Langone Health, New York, NY, United States; Christopher M.. Pruitt, Medical University of South Carolina College of Medicine, Charleston, SC, United States; Andrea T. Cruz, Baylor College of Medicine, Houston, TX, United States; Michelle Pickett, Medical College of Wisconsin, Milwaukee, WI, United States; Jaya CW. Ruffin, University of South Carolina School of Medicine Columbia, Columbia, SC, United States; Natalie J. Tedford, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States; Avani Bellary, American Family Children's Hospital, Madison, WI, United States; Emily Hogikyan, Medical College of Wisconsin, Milwaukee, WI, United States; Kersten Bond, Children's Hospital of Michigan, Detroit, MI, United States; Zachary Foughty, Baylor College of Medicine, Houston, TX, United States; Mohsen Saidinejad, University of California, Los Angeles David Geffen School of Medicine, Torrance, CA, United States; Deborah R. Liu, Keck USC School of Medicine, Los Angeles, CA, United States; Elizabeth Collins-Dippel, Children's Hospitals and Clinics of Minnesota, Minneapolis, MN, United States; M. Jennifer Abuzzahab, Children's Hospitals and Clinics of Minnesota - St. Paul, St Paul, MN, United States; Petter Bjornstad, University of Washington School of Medicine, Seattle, WA, United States
Pediatric Emergency Physician, Emergency Research Director Children's Minnesota Minneapolis, Minnesota, United States
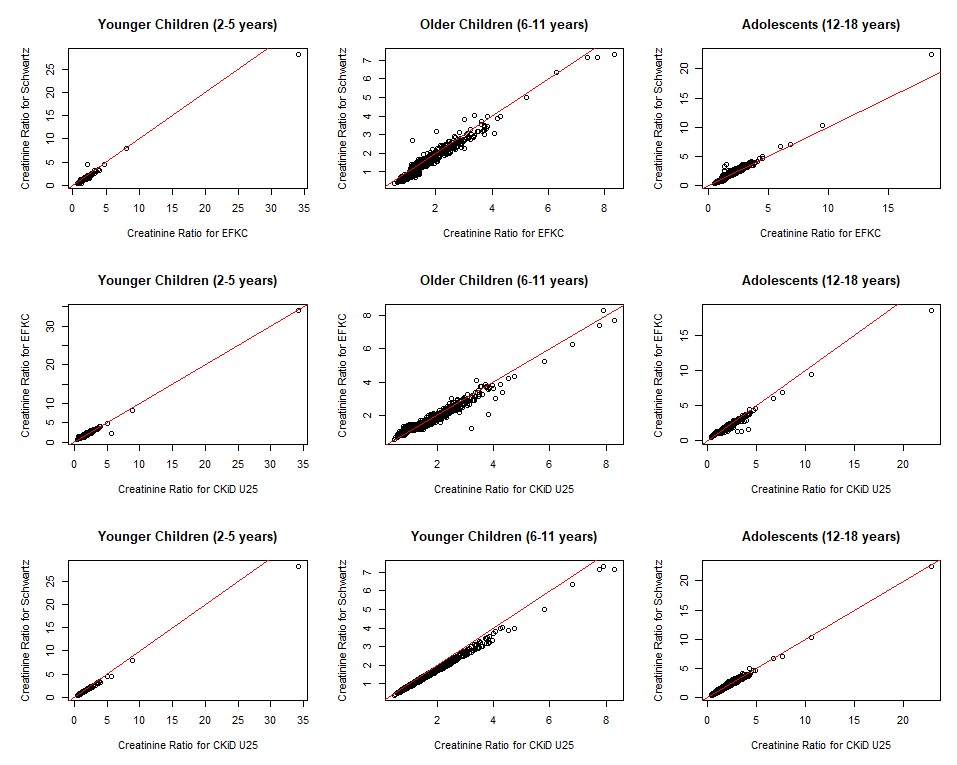
Background: Acute kidney injury (AKI) occurs in an estimated 40% of children with diabetic ketoacidosis (DKA). Baseline serum creatinine (sCr) is often unavailable; estimation is typically performed using the revised Schwartz (rSchwartz) equation. Comparisons with other equations estimating baseline kidney function are limited. Objective: Our primary aim was to compare AKI estimates in pediatric DKA using the rSchwartz, Chronic Kidney Disease in Children Under 25 (CKiD U25), and European Kidney Function Consortium (EKFC) equations. Our secondary aim was to assess AKI differences by age and baseline estimated glomerular filtration rate (eGFR). Design/Methods: We performed a multicenter, retrospective, cross-sectional study of children aged 2-18 years diagnosed with DKA between January 1, 2020 and December 31, 2023 at 9 participating emergency departments (EDs). The primary outcome was presence of AKI at any point during the encounter. AKI status was determined by observed/expected sCr ratios using the rSchwartz, CKiD U25, and EKFC equations. Analysis was stratified by age and eGFR. The Pearson Chi-Square test was used to compare AKI determination across estimating equations. Agreement in AKI determination for each level of eGFR was assessed by Fleiss' Kappa, and pairwise combinations of estimating equations were plotted by age group. Results: A total of 3487 encounters were analyzed [median age 12 years (IQR 10, 15); 51.5% female] (Table 1). Median time to first intravenous fluid bolus was 40 minutes (IQR 22, 75), and median time to first insulin was 132 minutes (92, 191). AKI assignment varied by equation (Figure 1), with EKFC identifying more AKI in younger children (8.2% vs. 5.5%) and CKiD U25 identifying more AKI in females (54.4% vs. 47.5%) compared to rSchwartz (Table 2). For each assumed eGFR (90, 100, 110, or 120 mL/min per 1.73m2), agreement between the three equations was high, and demonstrated no observable differences in AKI determination (kappa range = 0.79-0.82).
Conclusion(s): AKI determination in pediatric DKA varies by equation, age, and sex, but not by assumed baseline eGFR. These data suggest that assumed baseline eGFRs of 90-120 mL/min per 1.73m2 are reasonable. Further research should explore equation-specific criteria.
Demographics and encounter characteristics for encounters with DKA.
Scatter plots comparing the relationship between rSchwartz, CKiD U25, and EFKC for estimating the ratio of observed/expected serum creatinine (AKI), by age group.
Number of encounters classified as having AKI using the rSchwartz, CKiD U25, and EFKC equations, by age, sex, and eGFR.

 photo")
.jpg)
.jpg)
