444 - Utilizing a Transcutaneous Bilimeter to Decrease Lab Draws for Neonatal Jaundice in a Pediatric Emergency Department
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4435.444
Brittany Voth, Rady Children's Hospital San Diego, San Diego, CA, United States; Shelley Sherman Zapata, Rady Children's Health San Diego, San Diego, CA, United States; Amy Bryl, University of California, San Diego and Rady Children’s Hospital San Diego, San Diego, CA, United States; Yvette Wang, Rady Children's Hospital San Diego, San Diego, CA, United States
Chief Resident UC San Diego and Rady Children's Hospital San Diego San Diego, California, United States
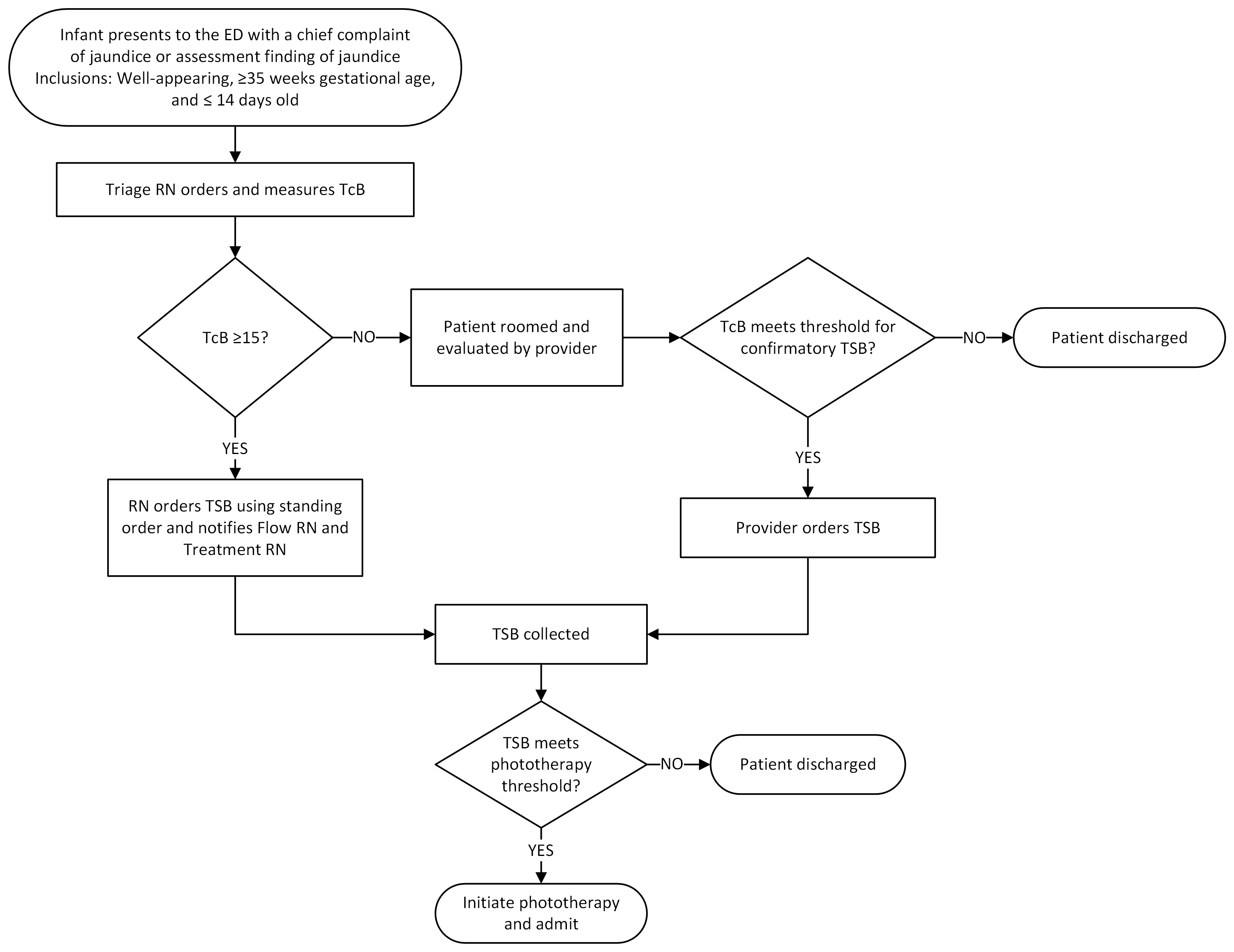
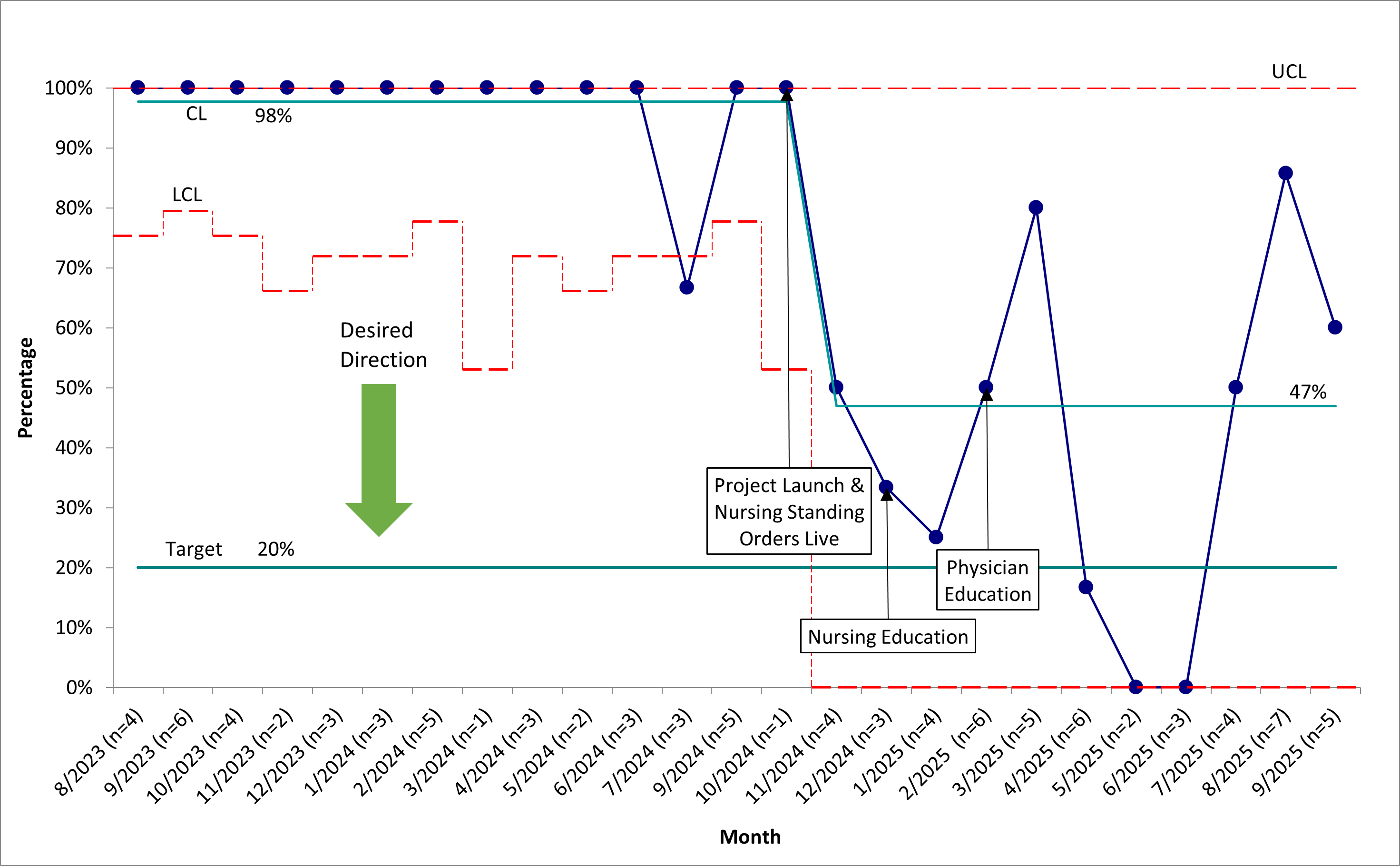
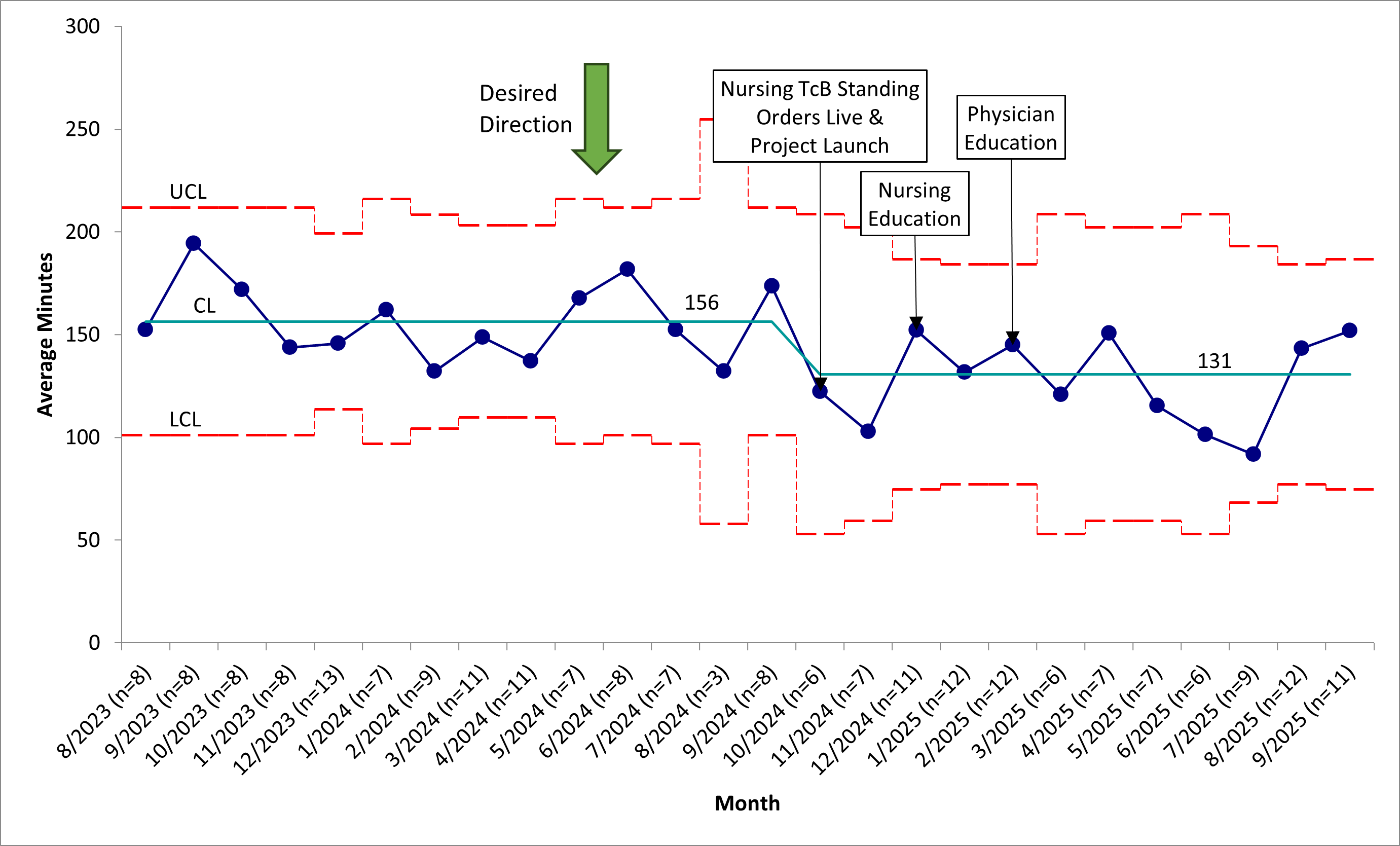
Background: Jaundice is one of the most common reasons for a neonate to present to an emergency department (ED). Many hospitals, including ours, use total serum bilirubin levels (TSB) to assess whether infants require admission for phototherapy. TSB requires a blood draw and testing, which can be stressful for the baby and parents, costly, and time-consuming. Transcutaneous bilirubin (TcB) is an accurate, non-invasive, and cost-effective strategy to screen for hyperbilirubinemia and the need for a confirmatory TSB. Objective: This global aim of this quality improvement (QI) project was to streamline the care of well-appearing infants at least 35 weeks gestation and age 14 days and younger presenting to the ED with jaundice. The SMART aim was to decrease the percentage of patients with TcB levels below threshold for confirmatory TSB testing who have labs drawn from 100% to 20% in 12 months. Design/Methods: Our multidisciplinary team created a process map and key driver diagram to determine areas of intervention (Figure 1). To promote measuring TcB in triage, we created a nursing standing order to obtain a TcB for infants 14 days and younger with jaundice, and if TcB was 15 mg/dL or higher, we created a standing order for nursing to order a confirmatory TSB. Other interventions included educating our nursing staff on this process and ED physicians on TcB interpretation. Our primary measure was the percentage of patients below the confirmatory TSB threshold with labs drawn. For discharged patients, an additional outcome measure was ED room to discharge time. Our process measure was the percentage of patients who had a TcB measured. Balancing measures included ED return visits within 3 days for jaundice. We used statistical process control to monitor changes in measures over time. Results: The proportion of infants with TcB levels below the confirmatory TSB testing threshold who had labs drawn decreased from 100% to 47% (Figure 2). ED room to discharge time decreased from 156 to 131 minutes (Figure 3). The percentage of patients who had a TcB measured increased from 47% to 85%. We did not observe a change in the percentage of patients returning to the ED within 3 days for jaundice.
Conclusion(s): Using QI methodology, we decreased the use of lab draws in the evaluation of well-appearing infants with jaundice. With the creation of nursing standing orders to streamline the process of measuring TcB and ordering confirmatory TSB testing, we decreased the room to discharge time of these infants by 25 minutes.
Figure 1: Process map for the evaluation of neonatal jaundice in the emergency department
Figure 2: Percentage of patients below confirmatory threshold with labs drawn by month
Figure 3: Average room to discharge time for discharged patients

 Credit")
 photo")