360 - Hospital utilization in children with medical complexity before and after enrollment in a tertiary care complex care program
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4353.360
Jimin Lee, Weill Cornell Medicine, New York, NY, United States; Daniela P. Nilo, NewYork-Presbyterian Morgan Stanley Children's Hospital, New York, NY, United States; Michael Rinke, The Children's Hospital at Montefiore, Bronx, NY, United States; Arti D. Desai, University of Washington School of Medicine, Seattle, WA, United States; Erika Abramson, Weill Cornell Medicine, Rye Brook, NY, United States; Madeline Sterling, Weill Cornell Medicine, New York, NY, United States; Divya Lakhaney, Columbia University Irving Medical Center, New York, NY, United States
Assistant Professor Weill Cornell Medicine New York, New York, United States
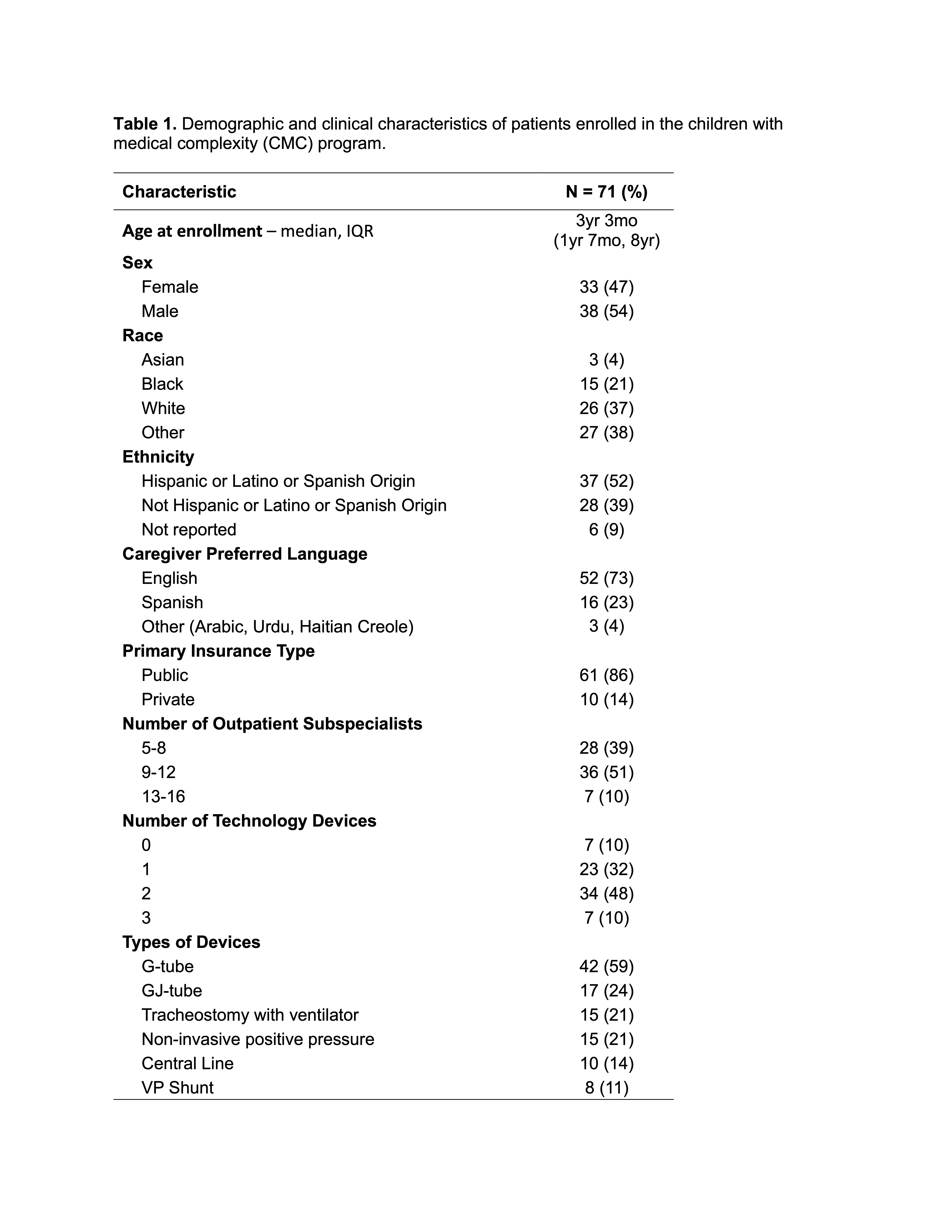
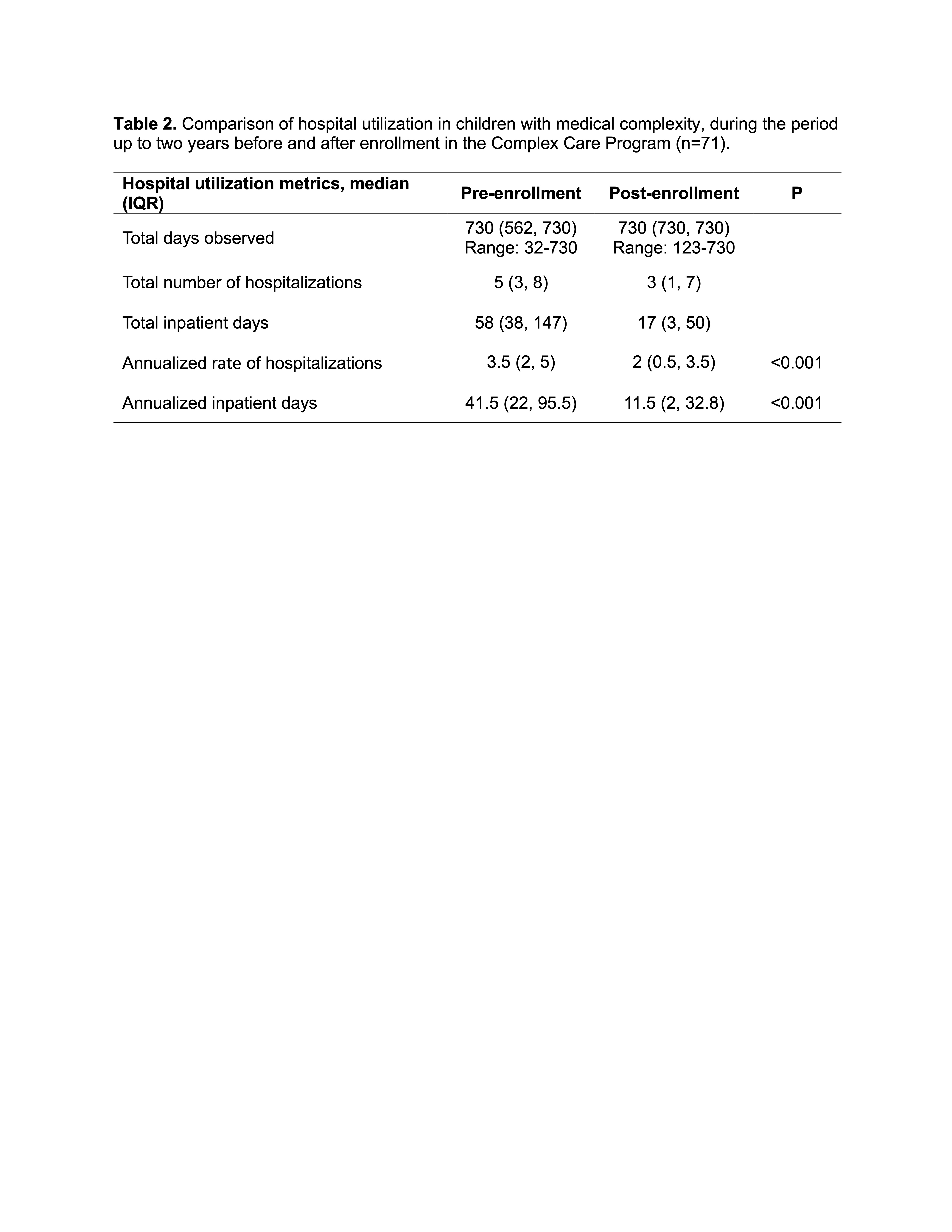
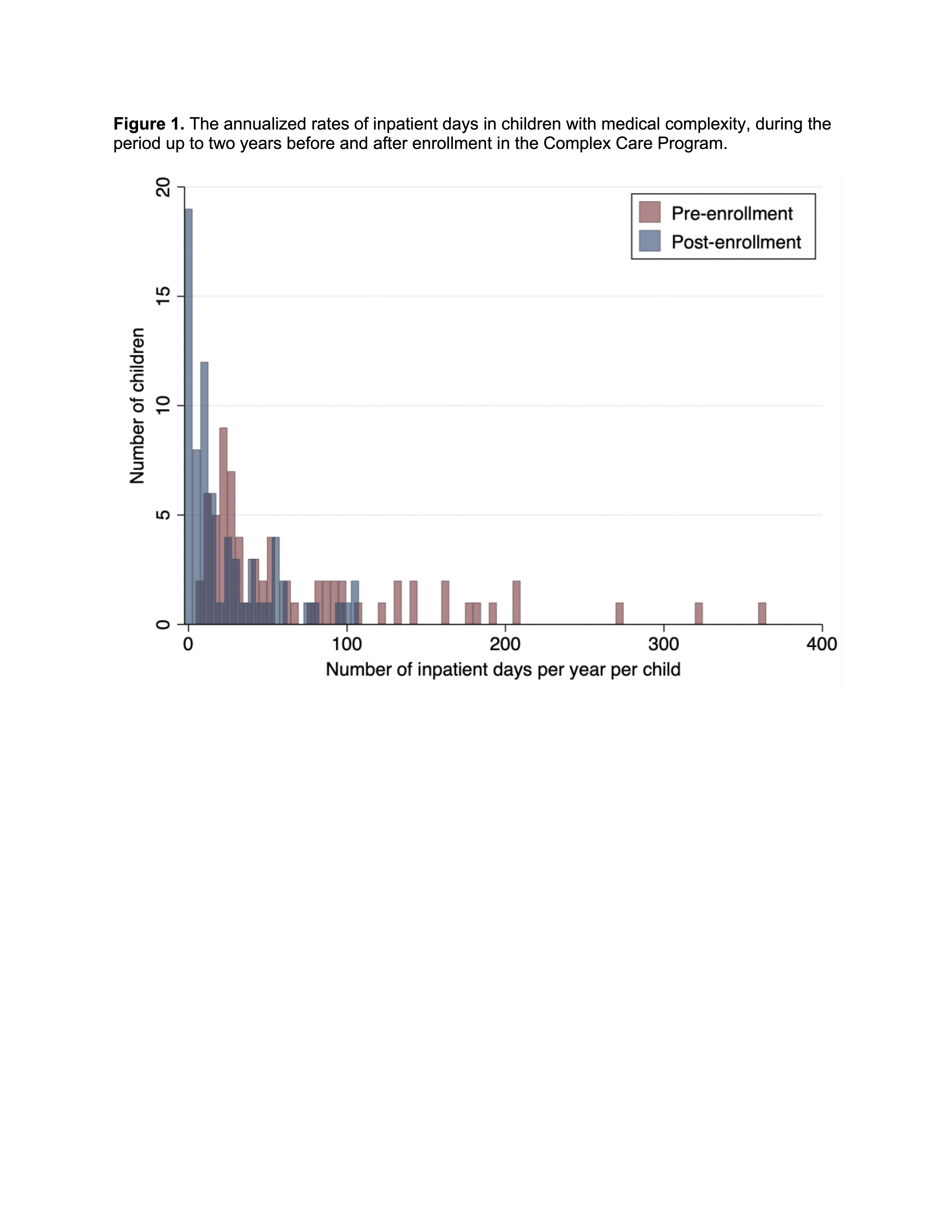
Background: Children with medical complexity (CMC) require coordinated care across multiple subspecialists and settings, yet evidence on the effectiveness of CMC-specific programs in reducing healthcare utilization is mixed. In 2015, we established the Complex Care Program (CCP) at an urban, academic, tertiary care center to serve predominantly low-income, racially diverse CMC families. The CCP integrates inpatient and outpatient care, provides a single point of contact, employs a bilingual community health worker, and develops individualized care plans to enhance continuity of care and reduce hospitalizations. Objective: To evaluate whether enrollment in the CCP reduces annualized rates of hospitalizations and inpatient days in CMC. Design/Methods: We conducted a retrospective cohort study of CMC patients enrolled in the CCP from 2015 to 2024, identified by ≥4 outpatient subspecialists and ≥20 inpatient days in the prior two years. Data were extracted from electronic health records. Demographic data included age, sex, race/ethnicity, preferred language, insurance, medical technology devices, and subspecialist count. Hospital utilization data were collected for up to 2 years pre- and post-enrollment until December 2024, or from birth for patients enrolled before age 2. Primary outcomes were annualized rates of hospitalizations and inpatient days, calculated as events or days divided by observation time in years. Patients with < 2 years of data were included using available observation time. Descriptive statistics were used to summarize patient characteristics. Wilcoxon matched-pairs signed-rank tests were used to compare pre- and post-enrollment rates. Results: Among 71 enrolled patients (median age 3y 3m, interquartile range (IQR) 1y 7m-8y), 54% were male, 86% had public insurance, 21% were Black, and 52% were Hispanic/Latino (Table 1). Patients had high medical complexity; 61% were followed by ≥9 outpatient subspecialists, and 58% used ≥2 medical technology devices. Median annualized hospitalization rates decreased from 3.5 (IQR 2.0-5.0) to 2.0 (IQR 0.5-3.5) per year post-enrollment (p < 0.001, Table 2). Similarly, median annualized inpatient days decreased from 41.5 (IQR 22-95.5) days to 11.5 (IQR 2-32.8, p < 0.001, Fig. 1).
Conclusion(s): CMC enrolled in the CCP had significantly fewer hospitalizations and number of inpatient days in the post-enrollment period. Limitations include the single-center, retrospective design without a control group, which limits generalizability. Future studies should assess cost-effectiveness and scalability in diverse settings.