571 - A clinical prediction model using novel predictors can discriminate risk of obesity at ages 2 and 5
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4559.571
Charles T. Wood, Duke University School of Medicine, Durham, NC, United States; Tracy Truong, Duke University School of Medicine, Durham, NC, United States; Jessica G. Woo, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Benjamin Goldstein, Duke University School of Medicine, Durham, NC, United States; Cindy Green, Duke University School of Medicine, Raleigh, NC, United States
Associate Professor of Pediatrics Duke University School of Medicine Durham, North Carolina, United States
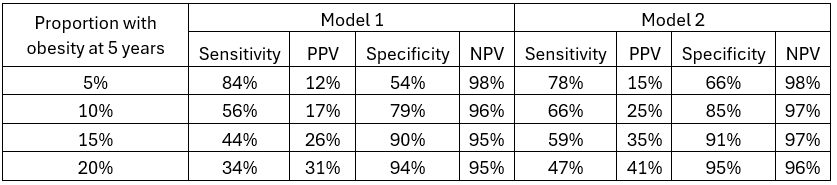
Background: Predicting which children are most likely to develop obesity in early childhood is critical for personalized, efficient care yet most models use data elements unavailable in electronic health record systems (EHR) or employ machine learning methods that lack interpretability. Objective: To develop models predicting obesity (body mass index [BMI] ≥ 95%) at ages 2 and 5 using predictors available in the EHR. Design/Methods: We used longitudinal outpatient data from 22,028 term infants born between 2017 and 2022 in one health system. Weight and length measures were cleaned with growthcleanr, an automated algorithm developed specifically for pediatrics. We excluded infants with weights < 2 kg and those with complex chronic diagnoses per existing Pediatric Medical Complexity Algorithm (PMCA). Model 1 included predictors commonly available in EHRs: maternal pre-pregnancy BMI; sex; birth weight; gestational age at birth; race; ethnicity; and insurance type. Model 2 added several derived predictors available in our EHR: breastfeeding duration, peak weight velocity, peak height velocity, peak infancy BMI, and age at these peaks. Regularized regression models based on least absolute shrinkage and selection operator (LASSO) were used to identify key predictors. We report optimism-corrected area under the receiver operating curve (AUC) and 95% CIs via 500 bootstrap samples as well as calibration slopes, a measure of accuracy of predicted risk. Comparison of AUC between 2 models was conducted using Delong's test. Results: Among 1766 infants (48% White, 22% Black, 16% Hispanic) with available data for both models, mean birth weight was 3370g (±443g), 50% were exclusively breastfeeding at 4 months, and 6.6% and 7.2% had obesity at 2 and 5 years, respectively. Model 1 had an AUC of 0.61 for obesity at 2 years and 0.72 at 5 years. Addition of breastfeeding, peak weight and height velocity, and peak infancy BMI significantly improved prediction, with model 2 AUCs of 0.88 and 0.73 for obesity at 2 and 5 years, respectively. Higher maternal pre-pregnancy BMI and higher peak infancy BMI were consistently associated with childhood obesity risk. (Table 1) Using US prevalence, our models provide high sensitivity and negative predictive values of 98-99%. (Tables 2 and 3).
Conclusion(s): Adding novel growth characteristics and feeding data to 7 traditional predictors of childhood obesity improved discrimination (AUC 0.88) and demonstrated moderate-to-good predictive performance. Implementation of our prediction model could identify those at highest risk childhood obesity using EHR data available in the first year of life.
Table 1. Significant predictors and AUC for each model and timepoint
Table 2. Test characteristics of prediction of obesity at 2 years at various thresholds
Table 3. Table 2. Test characteristics of prediction of obesity at 5 years at various thresholds

.png)
.png)