145 - Evaluating the Impact of Positive Reinforcement and Improved Transparency on Resident Satisfaction with the Back-Up Coverage System
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4142.145
Rachel L. Rothstein, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Sandrene J. Cassells, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Sivan Stein, Childrens Hospital of Philadelphia, Merion Station, PA, United States; Erin Tully, UPHS, Philadelphia, PA, United States; Kaylie Shojaie, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Jeanine Ronan, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Bryn M. Carroll, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Pediatric Emergency Medicine Fellow Childrens Hospital of Philadelphia Philadelphia, Pennsylvania, United States
Background: Residency back-up coverage is critical to maintaining resident wellbeing, hospital staffing and patient safety. Physicians have a history of presenteeism, attributed to patient care obligations, fear of negative perceptions and pressure to repay colleagues. Limited literature exists on resident perspectives and optimal structure of back-up coverage. Objective: To examine the impact of a new back-up coverage system, grounded in positive reinforcement and improved transparency, on resident satisfaction, call out volume and didactic attendance. Design/Methods: This prospective cohort study included pediatric residents at a large free-standing academic children's hospital. The historic back-up system was point-based, whereby residents lost points when calling out and gained points when called in for a shift. Residents were subsequently called in for coverage needs based on their net points.
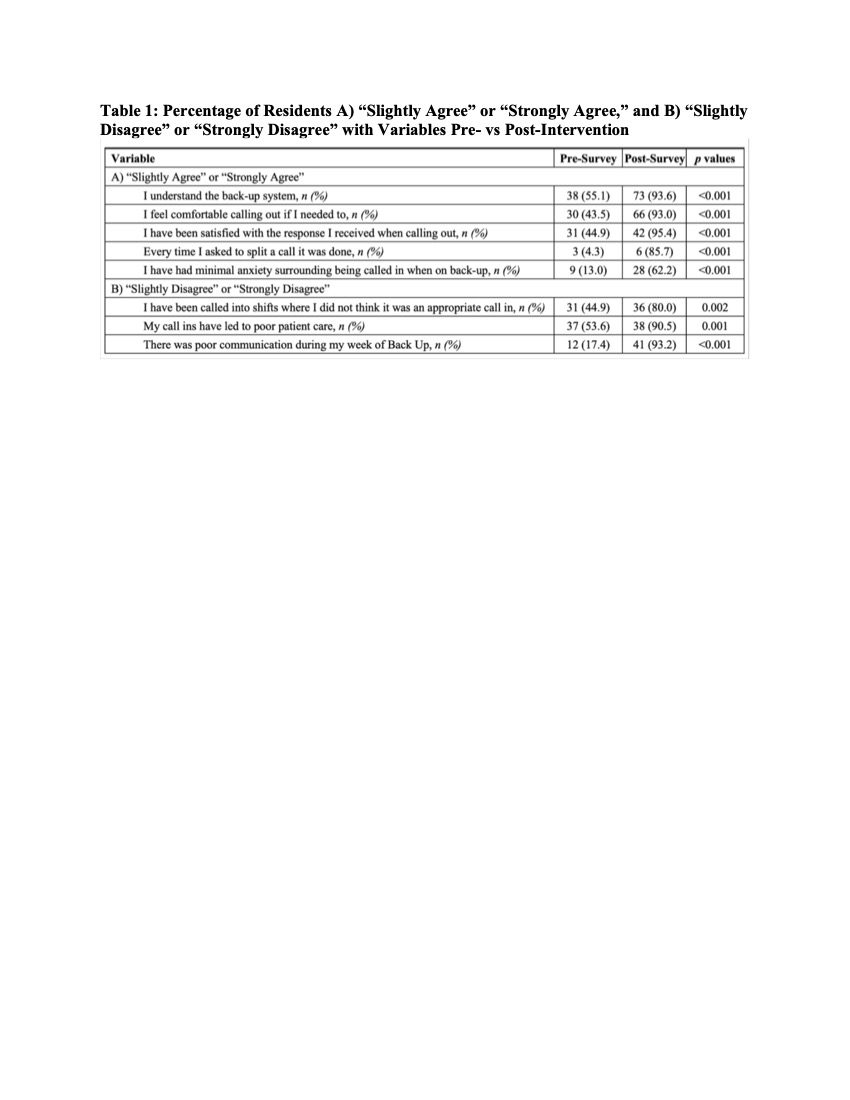
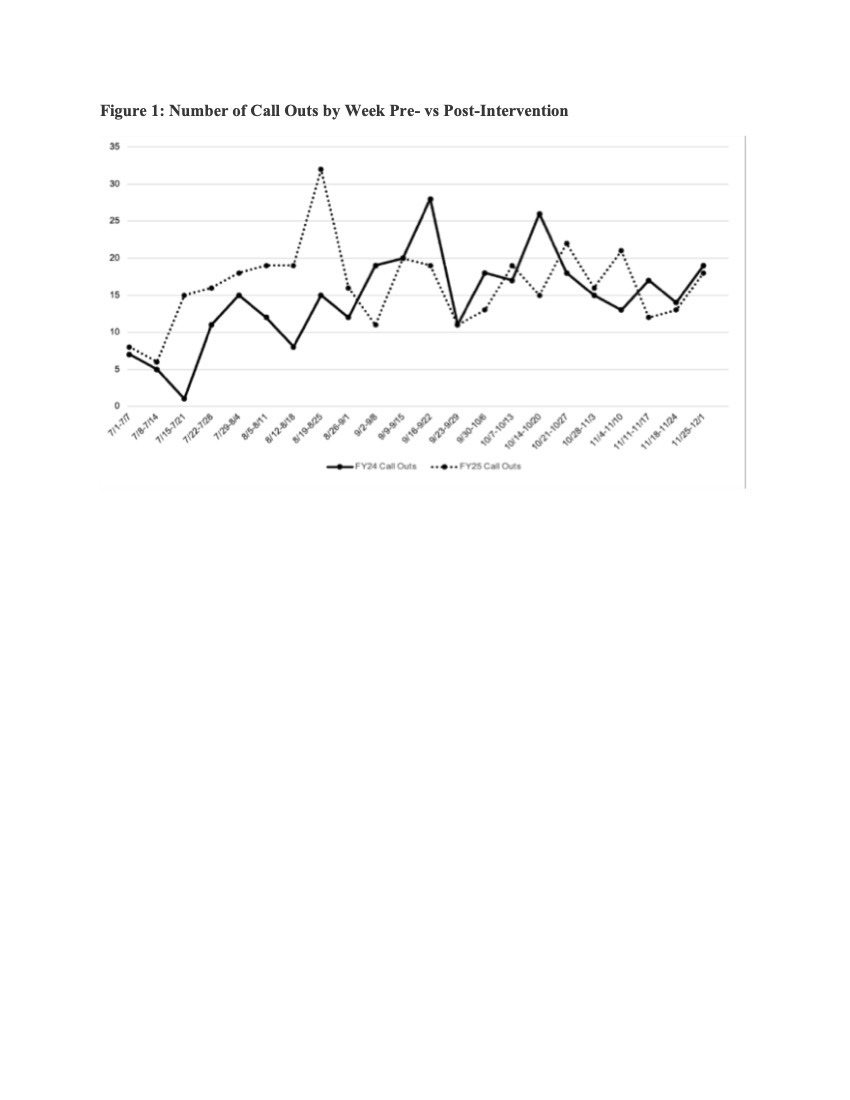
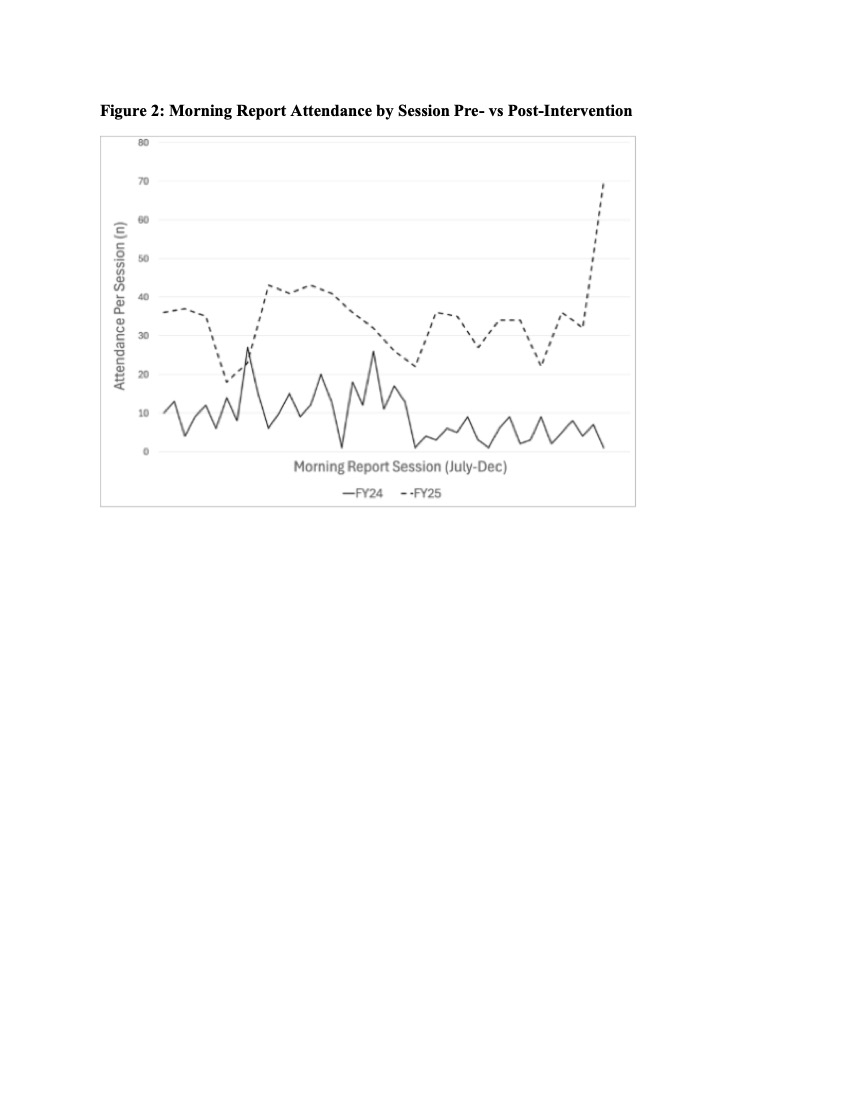
Residents engaged in a social contract exercise to discuss the purposes of back-up, the optimal call out/in process and methods of accountability. A resident-driven policy subsequently emerged, with the following adjustments to the historical system: Residents 1) No longer lost points for calling out, 2) Gained bonus points for attending morning report, 3) Received daily texts regarding known coverage needs and resident call in order and 4) Split 24-hour call coverage needs with a second resident upon request if staffing permitted. Pre- and post-intervention surveys with Likert items evaluated resident impressions of these changes, with comparisons made using a two-sample test of proportions and t-tests. Results: We observed a significant increase pre- vs post-intervention in the percent of residents "slightly" or "strongly" agreeing that they: 1) Understand the back-up system, 2) Feel comfortable and satisfied with the response when calling out, 3) Have minimal anxiety about being called in and 4) Have had calls split with another resident upon request (Table 1). We observed a significant increase in the percent "slightly" or "strongly" disagreeing that: 1) They have been called in for shifts they did not think were appropriate, 2) Call ins have led to poor patient care and 3) Communication during back-up was poor (Table 1). No significant difference was observed in the average number of call outs per week (14.6 vs 16.3, p=0.34, Figure 1). Average attendance per morning report session significantly increased (9.0 vs 34.2, p< 0.01, Figure 2).
Conclusion(s): Our new system demonstrated favorable impacts on resident perceptions of back-up and improved attendance at didactics, without significantly increasing call out volume.
Table 1: Percentage of Residents A) "Slightly Agree" or "Strongly Agree," and B) "Slightly Disagree" or "Strongly Disagree" with Variables Pre- vs Post-Intervention
Figure 1: Number of Call Outs by Week Pre- vs Post-Intervention
Figure 2: Morning Report Attendance by Session Pre- vs Post-Intervention

 photo")