763 - Breaking the Habit: A Quality Improvement Initiative to Eliminate Gastric Residual Checks in the NICU with Nursing Insights
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1739.763
Mohammad Adawi, University of Florida College of Medicine, Jacksonville, FL, United States; Matthew Garber, University of Florida College of Medicine, Jacksonville, FL, United States; Padma Nandula, Unive, Jacksonville, FL, United States; Vasantha HS. Kumar, University of Florida College of Medicine, Jacksonville, FL, United States; Sanket Shah, University of Florida College of Medicine, Jacksonville, FL, United States
Assistant Professor University of Florida College of Medicine Jacksonville, Florida, United States
Background: Routine gastric residual (GR) checks have long been used in NICUs to assess feeding tolerance and as a surrogate marker for feeding increment. However, evidence suggests that GR volume and color are poor predictors of necrotizing enterocolitis (NEC), potentially delaying feeding advancement and prolonging parenteral nutrition. Eliminating routine GR aspiration in favor of symptom-based assessments has been shown to improve feeding outcomes without increasing the incidence of NEC. Objective: This quality improvement (QI) project aims to align practice with current evidence by discontinuing routine gastric residual checks for preterm infants. Design/Methods: Setting: Level III NICU, University of Florida Health, Jacksonville. Population: Infants < 1500 grams birth weight. Primary
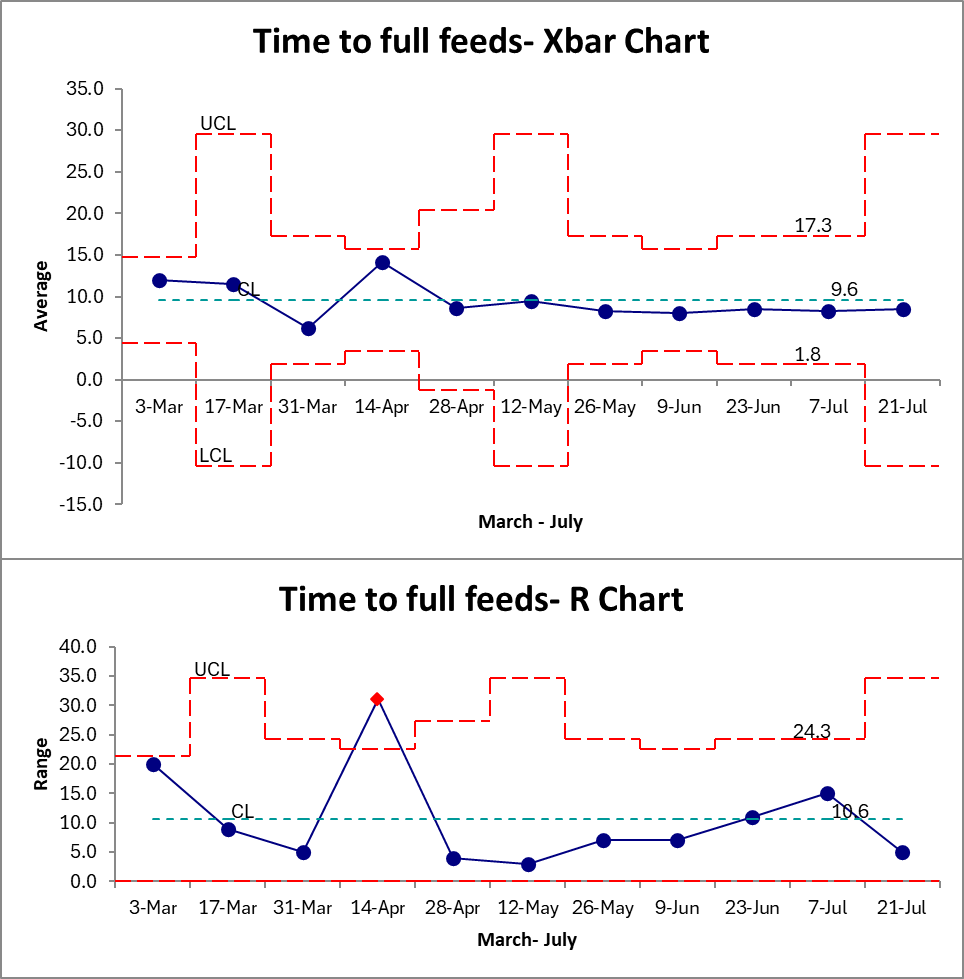
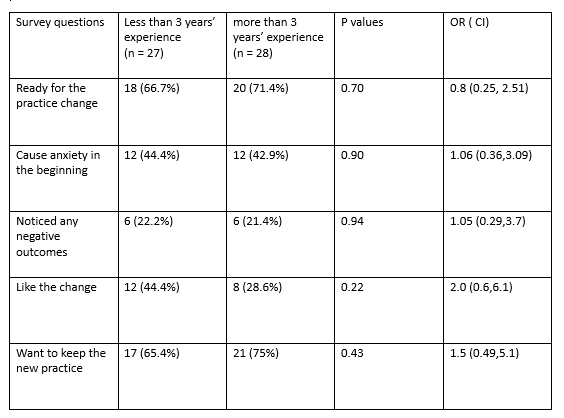
Aim: to eliminate routine gastric residual checks QI Strategy: • PDSA 1 (Jan-Feb 2025): Staff education on symptom-based feeding assessment. • PDSA 2 (Mar-Apr 2025): EPIC® order modification allowing GR checks only when clinically indicated. • PDSA 3 (May-Jun 2025): Reinforcement of nursing education. Outcome Measure: Rate of GR checks (U chart). Balancing Measures: NEC incidence, feeding intolerance, KUB imaging for abdominal symptoms, and time to full feeds. Post QI Nursing Survey: Conducted 6 months post-implementation to evaluate perceptions, comfort, and barriers. Results: 41 infants were eligible between March and July 2025. We achieved 100% compliance with no residual checks within 2 months of implementation of project (chart not shown due to rapid improvement). Average time to full feed remained stable at 9.6 days (figure 2). Additionally, we did not notice an increase in abdominal X-ray or feeding interruptions. A total of 55 nurses participated in the post-implementation survey (27 with less than 3 years of experience and 28 with more than 3 years). Most nurses in both groups reported being ready for the practice change (66.7% vs. 71.4%, p = 0.70) and wished to keep the new protocol (65.4% vs. 75%, p = 0.43). Although nurses with less experience were slightly more likely to report liking the change (44.4% vs. 28.6%), this difference was not statistically significant (p = 0.22). (Table 1)
Conclusion(s): We successfully implemented a new practice of eliminating residual checks in our NICU. Despite initial anxiety, nursing staff adapted quickly and supported sustainability of the change. This project demonstrates that a multidisciplinary approach and ongoing education facilitate culture change and improve practice consistency without compromising infant outcomes.
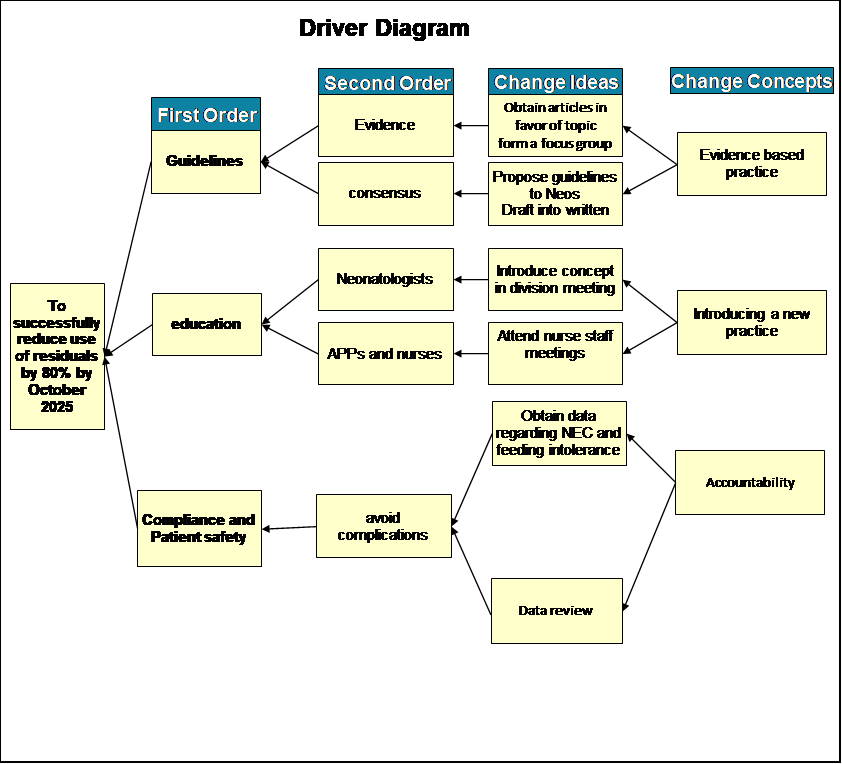
Figure 1: Key Drivers Diagram
Figure 2: Time to Full Feeds (Xbar Chart) and Variability in Feeding Time (R Chart) for Preterm Infants Before and After Elimination of Routine Gastric Residual Checks (March-July 2025)
Table 1: Post-QI Nursing Perceptions by Experience Level

 Credit")
 photo")