342 - Evaluation of Factors Associated with Readmission for Growth Faltering
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4335.342
Vandana Garg, UAMS/ACH, Little Rock, AR, United States; Liza Murray, University of Arkansas for Medical Sciences College of Medicine, Little Rock, AR, United States; Brittany Slagle, Arkansas Children's Hospital, Little Rock, AR, United States; Charalene Fisher, University of Arkansas for Medical Sciences College of Medicine, Little Rock, AR, United States; Emily Wilson, University of Arkansas for Medical Sciences College of Medicine, Little Rock, AR, United States; Bianca Rochelle, University of Arkansas for Medical Sciences College of Medicine, maumelle, AR, United States
Resident Physician UAMS/ACH Little Rock, Arkansas, United States
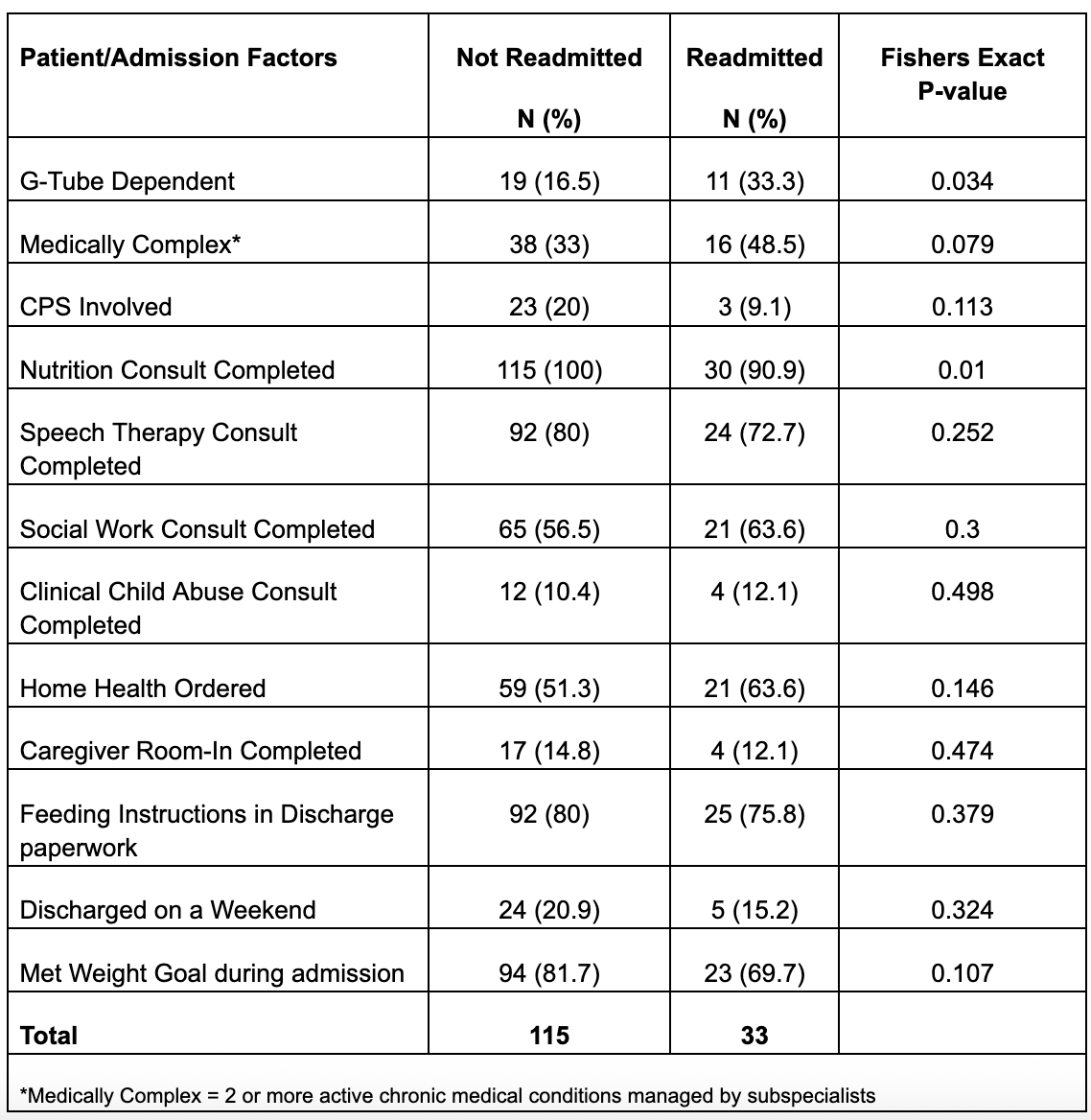
Background: This study was a part of a QI initiative to promote successful outpatient management evidenced by decreased readmissions for GF. Objective: The aim of this study was to identify factors associated with readmission for growth faltering (GF) within 6 months of an initial admission for GF. Design/Methods: This was a retrospective case-control study evaluating patients admitted between Jan 2023-Feb 2024. Patients were identified via EMR-generated list of admission diagnosis codes related to GF, failure to thrive or malnutrition. Patients diagnosed with an eating disorder were excluded. Cases were defined as patients readmitted for GF within 6 months of initial admission; controls were defined as those who were not. Patient factors included demographics, g-tube dependence, medical complexity, presenting complaints and child protective service involvement. Admission factors evaluated included completion of nutrition, speech therapy, and clinical child abuse team consults, caregiver completion of a room-in, goal weight gain demonstration during hospitalization, and feeding instructions in discharge paperwork. To control for loss to follow-up, comparative analysis was completed with patients who had a documented weight within 6 months of initial admission. Statistical analysis was completed by SPSS with Fisher's exact tests for categorical variables and ANOVA for comparison of means. Results: 148 of 186 identified admissions had a follow-up weight documented within 6 months; of these 33 (22.3%) patients were readmitted for GF. Excluding those without a documented follow-up weight, the average LOS for readmitted vs not readmitted was 13.8 days vs 6.0 days (p=0.10). A significantly larger proportion of readmitted patients were g-tube dependent (33.3% vs 16.5%, p=0.01) and there were a significantly smaller proportion of patients with completed nutrition consults in the readmitted group (90.9% vs 100%, p=0.03). 69.7% of readmitted patients demonstrated goal weight gain during initial admission vs 81.7% of those not readmitted (p=0.11).
Conclusion(s): Outpatient management of GF after hospitalization can be difficult as evidenced by our overall readmission rate of 17.7%. Patients with a g-tube may represent a high-risk group for readmission. While nearly all GF admissions had a nutrition consult, a smaller proportion of readmitted patients had one completed, supporting the necessity of a nutrition consult. Our study is limited by small numbers at a single institution; further study is needed to evaluate strategies for successful outpatient management of GF and identification of additional risk factors for readmission.
Table 1: Presence of Patient/Admission Factors in Readmitted Patients and Not Readmitted Patients, First Admissions

 photo")