312 - Dexmedetomidine Sedation in the NICU: Comparative Analysis of Liver Function Tests Before and After Administration
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4306.312
muppala Prasanth raju, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; Muktika Reddy Kalagiri, University of texas at austin, Temple, TX, United States; madhava (. Beeram, Baylor Scott and White Health, Temple, TX, United States; Kushi Shetty, University of Texas at Austin, Austin, TX, United States; Dozie Uzoma, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; Suleiman N. Essoh, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; Vandana Pothala, Baylor scott and white, Temple, TX, United States; Niraj Vora, Baylor Scott White McLane Children's Medical Center, Leander, TX, United States; Vinayak Govande, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States
Neonatal-Perinatal Fellow Baylor Scott White McLane Children's Medical Center Temple, Texas, United States
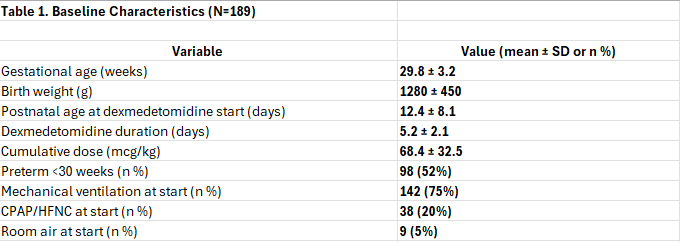
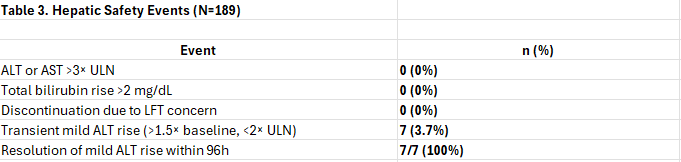
Background: Dexmedetomidine is increasingly utilized for sedation in the neonatal intensive care unit (NICU) due to its minimal respiratory depression, hemodynamic stability, and opioid-sparing effects, making it ideal for procedural sedation, and weaning from mechanical ventilation. However, as a hepatically metabolized agent (via CYP2A6 and glucuronidation), concerns persist regarding potential hepatotoxicity in neonates with immature liver function, especially preterm infants with physiologic cholestasis, prolonged parenteral nutrition, or sepsis. Objective: To comprehensively evaluate the hepatic safety of dexmedetomidine in neonates admitted to NICU through LFT monitoring before, and after infusion, with subgroup analyses by gestational age, exposure duration, and cumulative dose. Design/Methods: Retrospective cohort study (2020-2025) at a level IV NICU. Included 189 neonates (GA 24-36 weeks) receiving dexmedetomidine (0.2-0.7 mcg/kg/h) for ≥48 hours. LFTs (ALT, AST, total bilirubin) measured ≤24h pre-infusion (baseline) and within 24h post-infusion (after). Exclusions: congenital liver disease, baseline LFTs >2x ULN. Analysis was performed using Paired t-tests; P< 0.05 significant. Results: Baseline characteristics included Mean gestational age: 29.8 ± 3.2 weeks and a Mean birth weight: 1280 ± 450 g. 52% (98/189) were < 30 weeks gestation. Liver function test results demonstrated no statistically or clinically significant changes from pre-infusion (≤24h before start) to post-infusion (within 24h after discontinuation): ALT: 25.4 ± 8.1 U/L (before) → 26.8 ± 8.9 U/L (after); P = 0.16 AST: 38.6 ± 12.4 U/L (before) → 39.7 ± 13.0 U/L (after); P = 0.22 Total bilirubin: 4.2 ± 1.5 mg/dL (before) → 4.3 ± 1.5 mg/dL (after); P = 0.31, No evidence of hepatic injury. Only 3.7% had transient mild ALT rise, all self-resolved.
Conclusion(s): In 189 critically ill neonates-including 52% born < 30 weeks and across all respiratory support levels-dexmedetomidine was associated with no significant change in LFTs before vs. after infusion. Safety was consistent across gestational ages, infusion durations, and respiratory support levels, confirming very good hepatic tolerability of dexmedetomidine in routine NICU use.
Table 1. Baseline Characteristics (N=189)
Table 2. Liver Function Tests Before vs. After Dexmedetomidine (N=189)

.jpeg.jpg "Dozie Uzoma, MD (she/her/hers) photo")