74 - Increasing Firearm Screening in Resident Pediatric Well-Child Checks: A Quality Improvement Project
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4072.74
Tiffany Y. Chen, Children's Hospital Los Angeles, Los Angeles, CA, United States; William Butler, Children’s Hospital Los Angeles, Los Angeles, CA, United States; Tatiana Campuzano, Children's Hospital Los Angeles - Children's Hospital Los Angeles4650 Sunset Blvd., #170Los Angeles, CA 90027UNITED STATES - Los Angeles, CA, Los Angeles, CA, United States; Aashna Patel, Children’s Hospital of Los Angeles, Los Angeles, CA, United States; Archana Sivanandam, Children’s Hospital Los Angeles, Los Angeles, CA, United States; Jeffrey R. Birnbaum, Children's Hospital Los Angeles, Los Angeles, CA, United States
Resident Children's Hospital Los Angeles Los Angeles, California, United States
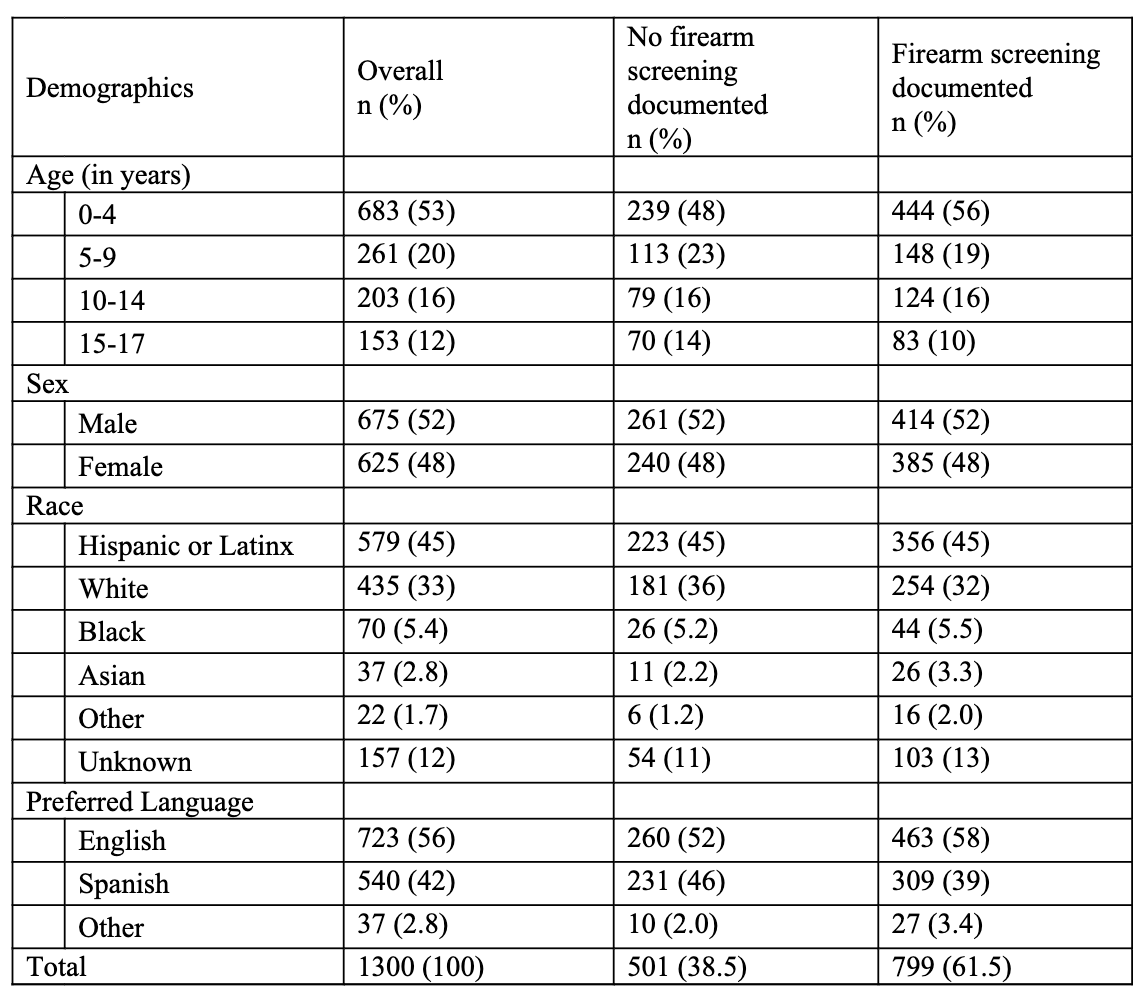
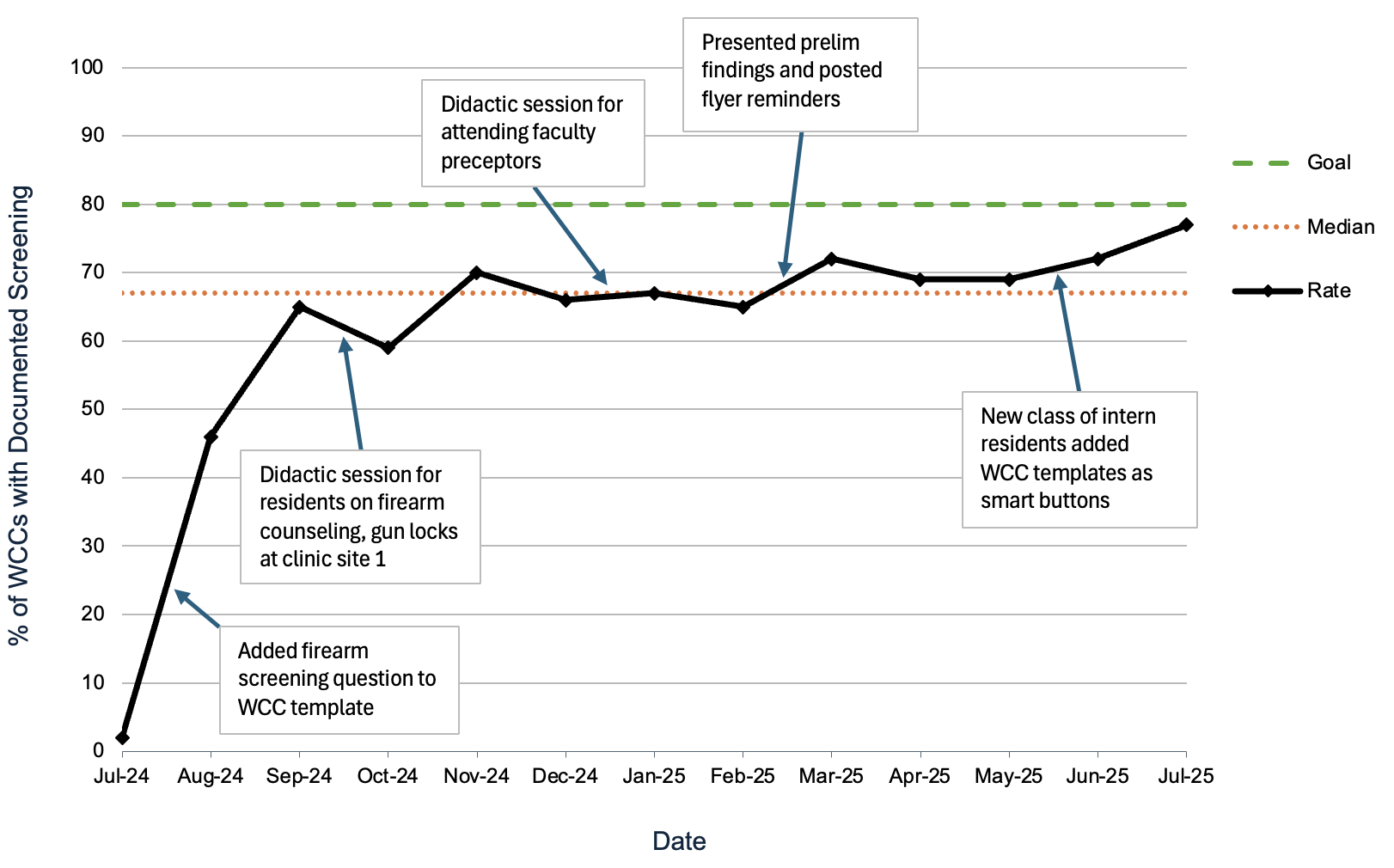
Background: Firearms are the leading cause of death among children and teenagers in the United States. They also cause significant morbidity, from lasting physical disabilities to adverse impacts on mental health. In 2021, an estimated 30 million children lived in households with firearms. Although the American Academy of Pediatrics recommends routine firearm screening and anticipatory guidance during well-child checks (WCCs), screening rates remain low. Objective: To increase firearm screening rates in pediatric resident WCCs at two urban academic clinics to 80% within 13 months and explore associations between patient demographics and reported firearm presence. Design/Methods: This project was deemed exempt by the Institutional Review Board. A series of interventions (Table 1) were implemented to promote firearm screening. Eligible encounters included patients aged 0 to 17 years old seen for WCCs with associated ICD-10 codes by pediatric residents at two clinics. We reviewed 100 randomly selected charts per month for demographics and screening documentation. The primary outcome was the rate of firearm screening, defined as the percentage of resident WCCs with documented screening. A run chart was used to display monthly screening rates. Results: Between July 1, 2024 and July 31, 2025, 1300 charts were reviewed. Of these, 61.5% had documented firearm screening (Table 2). Firearm screening rates increased from 2% at baseline to 77% at the end of the study period, with a median rate of 67% (Figure 1). The greatest improvement (2% to 46%) occurred after the first intervention when we added a firearm screening question to the WCC template. Firearm screening rates were maintained above the median for the last five months of the study period. Twelve patients (0.9%) screened positive for firearm presence in the home. This small number was insufficient for statistical analysis. Of these, 10 were English-speaking, 9 reported storing their firearms in locked safes, 5 reported keeping ammunition separate, and 2 reported that they had a family member in law enforcement.
Conclusion(s): Quality improvement can be an effective mechanism to increase firearm screening in pediatric WCCs, but further work must be done to determine sustainability. The lower-than-expected prevalence of firearm ownership reflects underreporting, possibly driven by privacy concerns and social desirability bias. Continued normalization of firearm safety discussions during WCCs may improve both reporting accuracy and safe storage counseling.
Table 1. Timeline of interventions
Table 2. Demographic characteristics by firearm screening documentation status
Figure 1. Rate of documented firearm screening per month from July 1, 2024 to July 31, 2025

 Credit")
.png)