Session: Neonatal Pulmonology - Clinical Science 6: PEEP and Non-Invasive Ventilation
696 - Optimal High CPAP pressure levels in preterm neonates post-extubation: A prospective randomized crossover study
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4680.696
Amit Mukerji, McMaster University, Hamilton, ON, Canada; Heather Johnson, McMaster University Michael G. DeGroote School of Medicine, Hamilton, ON, Canada; Anton van Kaam, Emma Children's Hospital Amsterdam UMC, Amsterdam, Noord-Holland, Netherlands; Jaques Belik, University of Toronto Temerty Faculty of Medicine, Toronto, ON, Canada; Jennifer Beck, UnityHealthToronto, Toronto, ON, Canada; Gerhard Fusch, McMaster University, Hamilton, ON, Canada; Lehana Thabane, McMaster University/St Joseph's Healthcare Hamilton, Hamilton, Ontario, Canada L8N 4A6, ON, Canada
Associate Professor McMaster University Hamilton, Ontario, Canada
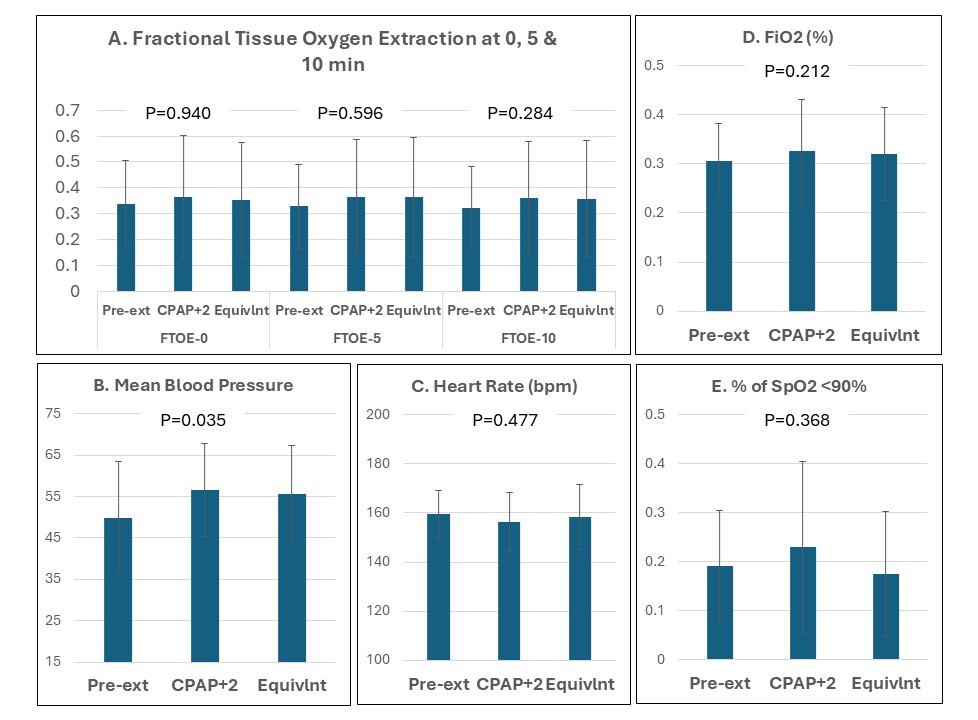
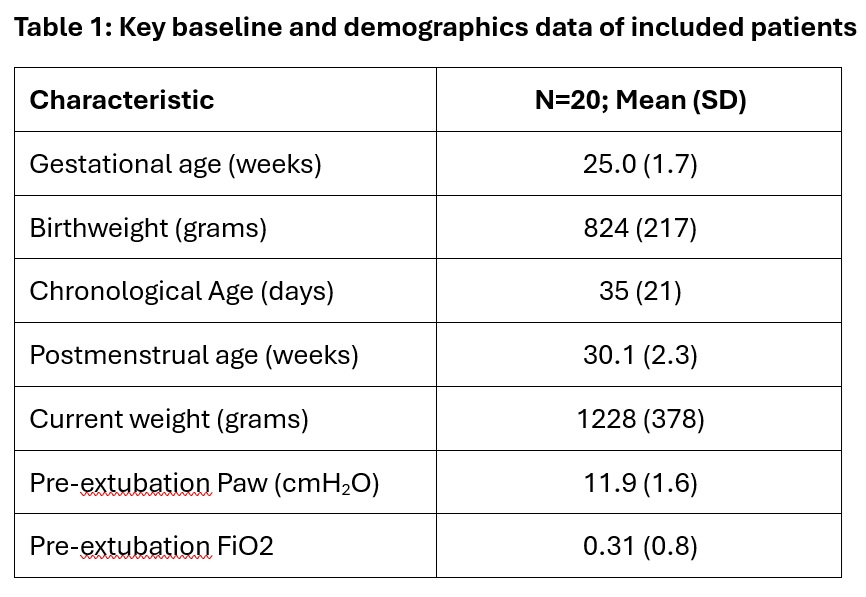
Background: Use of CPAP has traditionally been limited to 5-8 cmH2O; however, in recent years some emerging evidence suggests that use of high CPAP pressures ≥9 cmH2O may improve extubation success. However, the optimal post-extubation CPAP level, including in relation to physiological impact, remains unknown. Objective: To comparatively evaluate the short-term impact of two different high CPAP pressures when used as a post-extubation support mode in preterm neonates. Design/Methods: In this prospective randomized cross-over trial, preterm neonates < 29 weeks' GA and >7 days old being extubated from a mean airway pressure (Paw) of 9-13 cmH₂O were eligible. Each infant received CPAP 2 cmH₂O above (intervention) and equal to (control) their pre-extubation Paw for 1 hour each, in random order. The primary outcome was maximum diaphragmatic electrical activity (Edi), indicating effort to generate tidal volume. Secondary outcomes included minimum Edi (effort to maintain FRC), fractional tissue oxygen extraction, and other physiological measures. All parameters were recorded pre-extubation and during both study phases. Delivered Paw at the nasal interface was measured post-extubation. Data were analyzed using repeated measures ANOVA, with significance at P< 0.05. Results: Out of 23 enrolled infants, 20 completed the study without requiring intubation during the 2-hour study period. Baseline and demographic data of the included infants are shown in Table 1. The measured Paw pre-extubation was 11.9 (1.6) cmH2O, while the measured Paw at the nasal interface was 9.7 (1.4) and 8.3 (1.7) cmH2O for the intervention and control periods, respectively. The primary outcome of maximum Edi was not different across any of the study periods (Figure 1); however, the minimum Edi was lowest during CPAP+2 cmH2O (P=0.031). There were no differences noted in any of the additional outcomes; differences in mean blood pressure were statistically significant, but unlikely to be of clinical importance (Figure 2).
Conclusion(s): Use of CPAP pressures 2 cmH2O higher than pre-extubation Paw, compared to equivalent pressures, did not show any difference in maximum Edi but did show a small and statistically significant reduction in minimum Edi. These findings call for further evaluation of both physiological and clinical impact of CPAP+2 cmH2O in preterm neonates.
Table 1: Key Baseline and Demographics Data
Figure 1: Maximum and Minimum Edi during pre-extubation and both study periods
Figure 2: Additional physiological outcomes during pre-extubation and both study periods

.jpg)